

ABSTRACT
Gender-neutral vaccination (GNV) of human papillomavirus (HPV) may help reduce the transmission and incidence of HPV-related diseases. However, approximately 40 countries have implemented HPV GNV schedules. We systematically evaluated HPV GNV cost-effectiveness models from January 2008 to May 2024 using MEDLINE, Embase, and Cochrane to identify key drivers of cost-effectiveness results. Fifty-three publications were included, primarily from high-income countries. Vaccine coverage, price, protection duration, and discount rates impacted cost-effectiveness, with lower prices and protection against HPV-related diseases resulting in cost-effective results. Results in models that included adults (≥18 years) were mixed and dependent on price, inclusion of non-cervical HPV-related diseases, and age groups considered. We conclude that HPV GNV can be a cost-effective strategy for preventing HPV-related diseases. However, its cost-effectiveness is highly dependent on vaccine coverage, price, and inclusion of non-cervical HPV-related diseases in models. Further economic evaluations of HPV GNV in low- and middle-income countries are recommended.
KEYWORDS: Human papillomavirus, cervical cancer, screening, vaccination, intervention, cost-effectiveness, economic evaluation
Background
Human papillomavirus (HPV) is the most common sexually transmitted infection, with more than 80% of sexually active people acquiring HPV infection in their lifetime.1,2 Moreover, HPV infection is an etiological agent of several conditions, including cervical, vulvar, vaginal, anal, penile, head and neck, and oropharyngeal cancer, as well as genital warts.3,4 As of November 2024, the World Health Organization noted that there were 6 licensed HPV vaccines — 3 bivalent (2vHPV), 2 quadrivalent (4vHPV), and 1 nonvalent (9vHPV) – with at least 125 countries recommending HPV vaccination for adolescent girls and 47 countries also including boys.5 However, estimated global coverage rates for HPV vaccination at last dose by age 15 in 2023 were 15% in girls and 5% in boys.6
Adoption of gender-neutral vaccination (GNV) for HPV may help reduce transmission and cancer rates, promote gender equity, access to vaccines, and minimize vaccine misinformation and stigma.7–9 However, just over 40 high-income and upper-middle-income countries have implemented HPV GNV schedules. While previously published publication(s) have reviewed the cost-effectiveness of HPV vaccination, reviews specific to the cost-effectiveness of GNV are scarce.10,11 A prior systematic review of HPV models, which included 8 GNV-specific models, noted that GNV programs were cost-effective if vaccine coverage among females was low and if publication(s) included male-associated HPV diseases.12 To date, there have been no published reviews specific to HPV GNV economic models. Such a review can shed light on potential barriers to implementation, support recommendations for current immunization programs, and highlight the advantages of GNV for both males and females across countries with varying income levels. Therefore, this review aims to summarize the cost-effectiveness of HPV GNV models, as well as the key drivers of cost-effectiveness.
Methods
Search strategy and data sources
A systematic literature review (SLR) was conducted on October 12, 2021, to identify publication(s) published since January 1, 2008. Journal articles and conference abstracts were searched in MEDLINE, Embase, and Cochrane. Search terms included “HPV,” “vaccination,” “cost-effectiveness,” and “disease elimination” (Appendices A-D). On May 23, 2024, the SLR was updated to include recent evidence on GNV programs published since October 12, 2021.
Publication(s) selection and data extraction
Publication(s) selection criteria were organized in the PICOTS framework (Table 1). Notable PICOTS criteria included modeling publication(s) (e.g., cost-effectiveness publication(s) or Markov models) of GNV among children aged ≥9 years or more and adults who were vaccinated with 4vHPV or 9vHPV vaccine. Search hits were independently screened in a 2-tier screening process (title/abstract and full-text) by 2 reviewers, with adjudication from a third reviewer to resolve any discrepancies. Selection was conducted in DistillerSR for the original search and Microsoft Excel for the updated search, and reasons for exclusion were tracked at both screening phases.
Table 1.
PICOTS criteria.
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population(s) |
|
|
| Interventions |
|
Any interventions not specified under inclusion criteria |
| Comparisons |
|
Any comparisons not listed under the inclusion criteria |
| Outcomes | Cost-effectiveness of HPV vaccination
|
Any other outcome not specified under inclusion criteria |
| Time |
|
Publications published prior to 2008 |
| Publication(s) design |
|
Publication(s) designs not specified under inclusion criteria |
| Other |
|
|
Abbreviations: HIV+: human immunodeficiency virus positive; HPV DNA: human papillomavirus infection deoxyribonucleic acid; HPV, human papillomavirus; IPVC, International Papillomavirus Conference; LY, life-year; MSM, men who have sex with men; QALY, quality-adjusted life-year; PICOTS, population, intervention, comparators, outcomes, time, publication(s) design.
Data on model design (model type, perspective, time horizon, cost year, discount rates, inclusion of herd immunity), model inputs (vaccine and disease costs, currency, HPV-related cancer incidence and mortality rates, and proportion of cases attributed to HPV for both males and females), and model outputs (incremental costs, incremental cost-effectiveness ratios [ICERs], sensitivity analyses, and key drivers of uncertainty and value) were extracted into an Excel database. Country income levels were categorized according to World Bank classifications.13
Data analysis and reporting
Data from the included publications were reported and summarized descriptively. Per the publication(s) protocol, no statistical analyses, meta-analyses, or sensitivity analyses were conducted for this literature review. This manuscript followed the 2020 PRISMA checklist for SLR reporting.14
Publication(s) quality assessment
Two reviewers assessed the quality of economic evaluations using the HPV FRAME checklist15 and the ISPOR CHEERS checklist.16 Quality assessment was performed for all included publications except conference abstracts, as they contained insufficient methodological data to assess publication(s) quality.
Results
publication(s) characteristics
The original search yielded 1641 records after deduplication. A total of 1382 records were excluded at the title/abstract screening stage, primarily due to publication(s) design (n = 889), outcomes (n = 282), and population (n = 115). A total of 259 records were screened at the full-text stage, and 133 were excluded. N = 126 records regarding HPV vaccination programs were included for extraction, of which 36 publications focused on the cost-effectiveness of GNV programs. These were supplemented with an updated literature search of GNV publication(s), which identified 444 records. A total of 390 records were excluded during title/abstract screening, and 37 records were excluded during full-text review, most of which were publication(s) about eliminating cervical cancer. Seventeen records were included from the expanded search, resulting in 53 included GNV cost-effectiveness publications across both searches. The process of electronic searching is presented in the PRISMA flow diagram in Figure 1. Key publication(s) characteristics for included publications, as well as factors and limitations that impacted the results, are presented in Table 2.
Figure 1.
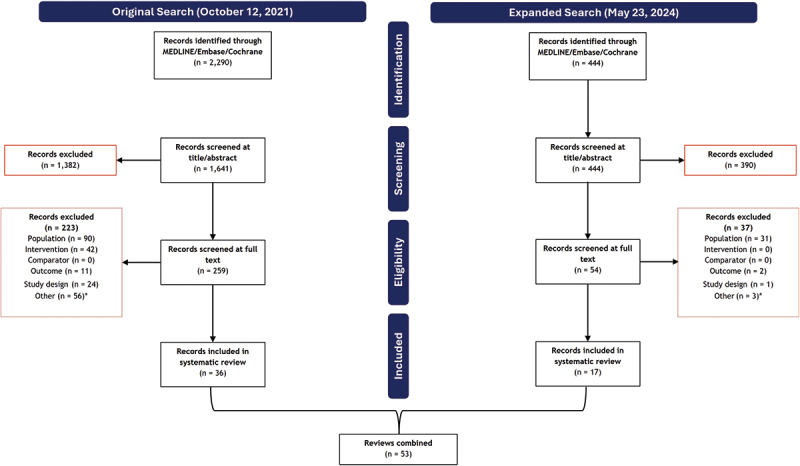
PRISMA flow diagram.
Table 2.
Summary of the results of the included studies.
| Geographic region | Author year | Population | Intervention | Comparator | Model used | Currency, year | Herd effects | Duration of vaccine protection | Vaccine coverage | Cancers included | Discount rates (cost/effects) | Factors impacting the results | Key limitations | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| South America | ||||||||||||||
| Brazil | Batista 202065 | 9- to 14-year-old females and 11- to 14-year-old males | 4vHPV GNV (high coverage) | 4vHPV GNV (low coverage) | Dynamic transmission | USD | Y | - | 1st dose: F: 80% M: 35% to 80% 2nd dose: F: 50% M: 35% |
CC, CIN1, CIN2+, GWs | 5%/5% | Coverage | NR | GNV was cost-saving at high coverage |
| Brazil | de Mendoca 202066 | 9- to 14-year-old females and 11- to 14-year-old males | 4vHPV GNV (high coverage) | 4vHPV GNV (low coverage) | Dynamic transmission | USD | Y | Lifelong | 1st dose: F: 80% M: 35% to 80% 2nd dose: F: 50% M: 10% to 50% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 5%/5% | Coverage, HPV-related cancers | NR | GNV was cost-effective at stable coverage and if all HPV-related cancers were considered |
| Colombia | Carrasquilla 202167 | 9- to 10-year-old males and females | 4vHPV GNV | 4vHPV FOV | Dynamic transmission | - | - | - | F: 35% to 50% M: 35% to 50% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | - | Coverage | NR | GNV was cost-saving at high vaccine coverage |
| Central America | ||||||||||||||
| El Salvador | Rendon 202268 | 9- to 10-year-old males and females | 4vHPV GNV | 4vHPV FOV | Dynamic transmission | - | Y | Lifelong | F: 65% to 80% M: 80% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | - | NR | GNV was cost-saving |
| Oceanic | ||||||||||||||
| New Zealand | Pearson 201454 | 12- to 13-year-old males and females | 4vHPV FOV/GNV current/enhanced coverage | No vaccination/4vHPV FOV/GNV current/enhanced coverage | Markov | NZ $, 2011 | Y | 20 years | F: 56% to 73% M: 56% to 73% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, VuC | 3%/3% | Cost | ● Model did not include different coverage rates for boys and girls, and the health benefits of cross-protection of the 4vHPV | GNV was not cost-effective unless the total cost/vaccination/individual was <NZ$ 375 |
| Asia | ||||||||||||||
| Vietnam | Sharma 201569 | ≥9 year-old males and females | 4vHPV FOV/GNV | No vaccination/4vHPV FOV | Dynamic transmission | INT$, 2008 | Y | Lifelong | F: 25% to 90% M: 25% to 90% |
CC, GWs | 3%/3% | Coverage, cost | ● Model did not incorporate the potential of vaccination to avert other HPV-related cancers ● Model assumed complete, lifelong vaccine efficacy |
GNV has marginal benefits over FOV. GNV is not cost-effective at vaccine cost >INT$ 5/dose if high vaccine coverage is achieved in FOV |
| Singapore | Tay 201746 | 11- to 12-year-old males and females | 4vHPV FOV/GNV ± CU (2/3 dose) | 4vHPV FOV | Mathematical | SGD, 2011 | N | Lifelong | F: 5% to 80% M: 80% |
CC, CIN1, CIN2+, GWs | 3%/3% | Coverage | ● No recorded data were available, so the model considered current HPV vaccine coverage rate in Singapore to be low ● The incidence of GW was probably underestimated as the data were based on cases diagnosed at sexually transmitted illness clinics ● Cases from general practitioners, obstetricians, gynecologists, and urologists were not included in the model, underestimating the benefits of 4vHPV ● Changes in cytology screening coverage could be a local factor that influenced the results. ● Coverage was assumed to be 50% |
GNV at 80% coverage was cost-effective over FOV at 5% coverage |
| Singapore | Varga 202234 | 13- to 14-year-old males and females | 9vHPV GNV | 2vHPV FOV | Dynamic transmission | SGD, 2018 | - | - | F: 92% M: 92% |
AC, CC, CIN1, CIN2+, GWs, PC, VaC, VuC | 3%/3% | - | NR | GNV was cost-effective |
| Singapore | Wahab 202339 | 13-year-old males and females | 2vHPV/9vHPV GNV | FOV | Static compartmental | SGD, 2021 | Y | - | F: 80% M: 80% |
AC, CC, H&NC/OPC, PC, VaC, VuC | 3%/3% | - | ● There may be limited generalizability to other countries as the assessment of cost-effectiveness is likely to be greatly influenced by the vaccine price, nationally negotiated with manufacturers | 2vHPV GNV was cost-effective |
| Japan | Palmer 202341 | 12- to 16-year-old males and females | GNV 9vHPV for females and 4vHPV for males | 9vHPV FOV | Dynamic transmission | USD, 2022 | - | - | F: 30% and 15% for CU M: 15% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | - | Coverage | ● The probability and timing of potential future programmatic changes to Japanese preventive health care were unknown and could not be accounted for in the model ● Only direct costs from the payer’s perspective were included; societal costs such as lost economic activity were not considered |
GNV was cost-effective if the current female vaccine coverage rate remains low (30%) |
| Türkiye | Akyol 202342 | 11- to 12-year-old males and females | 9vHPV GNV | No vaccination | Dynamic transmission | USD | - | - | F: 90% M: 90% |
AC, CC, H&NC/OPC, GWs, VaC, VuC | 3%/3% | - | NR | GNV with 9vHPV was very cost-effective |
| Hong Kong | Cheung 202344 | 12-year-old males and females | 9vHPV GNV ± CU | 9vHPV FOV | Dynamic transmission | HKD, 2019 | - | Lifelong | F: 70% and 30% for CU M: 70% and 30% for CU |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | - | ● The model did not include all the potential health or economic benefits of vaccination, likely underestimating the value of a routine GNV ● Model did not include disease transmission among MSM and possible changes to CCS over 100 years ● Input costs were derived from prices charged to a private case in a public hospital. The government heavily subsidizes prices charged to public cases; therefore, these prices do not reflect the actual costs The model assumed a high female vaccination coverage rate (70%), which may underestimate the true impact observed in a real-world setting Model may overestimate the number of deaths due to undiagnosed CC, thus overestimating QALYs gained and underestimating ICER due to deaths avoided |
GNV with 9vHPV was very cost-effective |
| South Korea | Park 202345 | 12-year-old males and females | 9vHPV GNV | 2vHPV/4vHPV FOV/No vaccination | Dynamic transmission | KRW | Y | Lifelong | F: 70% M: 50% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 1% to 3%/1% to 3% | - | NR | GNV with 9vHPV was cost-effective |
| Europe | ||||||||||||||
| Denmark | Olsen 201548 | 12-year-old males and females | 4vHPV FOV/GNV | No vaccination/4vHPV FOV | Agent-based transmission | EUR, 2008 | Y | Lifelong | F: 85% M: 85% |
CC, CIN1, CIN2+, H&NC/OPC, GWs | 3%/3% | Non-CC-related cases, dosing schedule, cost, coverage, discount rate, time horizon | ● Model considered only heterosexual transmission of HPV, 100% vaccine efficacy, and lifelong protection ● Model did not include naturally acquired immunity to HPV, future modification of the screening program and overall incidence of HPV related cancers (especially H&NC), leading to a marginal inaccurate estimation of future costs related to HPV vaccination ● Two different sources were used for the applied QALY weights for the general population and for specific occurrences/illnesses. QALY weights for the general population were distributed according to age group. This can lead to discrepancies and thus underestimate total gain in QALYs |
GNV with 4vHPV was cost-effective |
| Sweden | Wolff 201851 | 10- to 12-year-old males and females | 4vHPV GNV | 4vHPV FOV | Dynamic transmission | SEK, 2017 | Y | Lifelong | F: 80% M: 80% |
AC, CC, CIN1, CIN2+, H&NC/OPC, PC, VaC, VuC | 3%/3% | Price, coverage, discount rate | ● Dynamic HPV infection model was not used ● Model did not consider cross-protection and the added effect of 9vHPV ● Model did not consider differences in vaccination coverage or transmission patterns in other countries when calculating the effects of herd immunity |
GNV with 4vHPV was cost-effective, however, a lower vaccine price was favored |
| Norway | Diakite 202336 | 12-year-old males and females | 9vHPV GNV | 2vHPV GNV | Dynamic transmission | NOK, 2021 | - | Lifelong | F: 86% M: 84% |
AC, CC, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 2% to 4%/2% to 4% | Non-CC-related cases | ● The models were calibrated to the latest sociodemographic and epidemiological data available, which were sometimes derived from sources outside Norway. ● The models assumed a constant coverage rate in the new HPV DNA screening and vaccination programs and do not account for possible future changes in the screening and vaccination rates and their impact on the results |
GNV with 9vHPV was cost-effective |
| Norway | Burger 201450 | 12-year-old males and females | 4vHPV FOV/GNV | No vaccination/4vHPV FOV | Dynamic transmission | NOK, 2010 | Y | Lifelong | F: 71% M: 71% |
AC, CC, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 4%/4% | Price, coverage, discount rate | ● Model assumed the burden of HPV-related diseases remains constant over time while evidence suggests the incidence of OPC related to HPV may be increasing ● Transmission among MSM was not considered; this likely overestimated herd immunity conferred to males in a GOV ● Model did not account for any level of vaccine cross-protection ● Model did not allow for the potential of cross-border behavior, which may overestimate herd immunity |
GNV with 9vHPV was an attractive strategy; however, increasing FOV coverage was considered more cost-effective |
| UK | Datta 201927 | 12-year-old males and females | 2vHPV/4vHPV/9vHPV GNV | 2vHPV/4vHPV/9vHPV FOV | Epidemiological/transmission | £, 2013-2014 | Y | 20 years | F: 85% M: 85% |
AC, CC, H&NC/OPC, PC, VaC, VuC | 1.5% to 3.5%/1.5% to 3.5% | Coverage, discount rate | ● Model did not consider impact of future changes to screening technology, interval, and compliance | GNV with 2vHPV/4vHPV/9vHPV was cost-effective when a 1.5% discount was considered. However, increasing FOV coverage was considered more cost-effective |
| UK | Owusu-Edusei 202237 | 12- to 13-year-old males and females | 4vHPV GNV | 9vHPV GNV | Age-structured, deterministic, heterosexual, compartmental disease transmission | £, 2020 | Y | Lifelong | F: 77.5% to 88.1% F: 77.5% to 88.1% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 1.5% to 3.5%/1.5% to 3.5% | - | ● Model focused only on heterosexual transmission | GNV with 9vHPV was cost-effective |
| UK | Daniels 202230 | 13- to 14-year-old males and females | 9vHPV GNV (2 doses) | 9vHPV GNV (1 dose) | Dynamic transmission | £, 2019 | N | Lifelong | 1st dose: F/M: 4.45% and 2nd dose F/M: 84.55% or F: 89% M: 89% |
AC, CC, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3.5%/- | Price, coverage, discount rate, duration of protection | ● Model did not consider the indirect costs related to productivity losses ● Model calculated risk of HPV transmissible sexual contacts using the annual number of sexual partners for each age group, overestimating the risk of HPV transmission, especially among older populations ● The model does not account for recent updates to pre-vaccine era estimates of CC and other disease incidences, nor does the model account for changes in background cancer incidence |
GNV with 2-dose 9vHPV was cost-effective |
| UK | Song 202440 | 12- to 13-year-old males and females | 9vHPV GNV (2 doses) | 9vHPV GNV (1 dose) | Age-structured, dynamic | £, 2023 | - | 10 years to Lifelong | 1st dose: F/M: 80% and 2nd dose F/M: 70% |
AC, CC, H&NC/OPC, GWs, PC, VaC, VuC | 3.5%/3.5% | Price, coverage, discount rate, duration of protection | ● Model was limited to heterosexual HPV transmission, excluding dynamics between homosexual and heterosexual individuals | GNV with 1-dose 9vHPV was cost-effective |
| Ireland | Teljeur 201932 | 12-year-old males and females | 9vHPV/4vHPV FOV/GNV | No vaccination/4vHPV FOV | Cost-utility | EUR | - | - | - | - | - | Coverage | NR | 9vHPV GNV was cost-effective if the vaccine coverage was <78% in females |
| Austria | Boiron 201622 | 9-year-old males and females | 9vHPV GNV | 4vHPV GNV | Dynamic transmission | EUR, 2014 | Y | Lifelong | F: 60% M: 40% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | Price, discount rate, duration of protection | ● Model involved numerous parameters, and not all the needed parameters could be found from Austria-specific publication(s) ● CIN incidences and additional benefits of 9vHPV on CIN, VuC, and VaC were substantially underestimated ● Economic benefits of HPV vaccination were underestimated since the indirect effects of cancer were not considered ● Model focused on heterosexual transmission |
GNV with 9vHPV was cost-effective |
| Austria | Bresse 201447 | 9-year-old males and females | 4vHPV GNV | No vaccination | Dynamic transmission | EUR, 2012 | N | Lifelong/ 20 years | F: 65% M: 65% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | Coverage, discount rate | ● The increased incidence of OPC, AC, and PC observed over the past decades in Denmark, Sweden, and the UK might also be present in Austria but not taken to account, hereby underestimating the potential benefits among boys, and thus increasing the ICER | GNV with 4vHPV was cost-effective |
| Netherlands | Palmer 202438 | 9-year-old males and females | 9vHPV GNV ± CU | 2vHPV/9vGNV GNV | Dynamic transmission | EUR | - | - | F: 70% M: 50% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 1.5%/4% | Disease utility | NR | GNV with 9vHPV was cost-effective |
| Germany | Largeron 201717 | 12- to 17-year-old males and females | 9vHPV GNV/FOV | 4vHPV FOV | Deterministic SIRS | EUR, 2014 | Y | Lifelong | F: 16.3%-55.6% M: 16.3%-55.6% |
AC, CC, CIN1, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | Non-CC-related cases, discount rate, duration of protection | ● Model shows a significant underestimation on the incidence of both grades of CIN due to lack of German-specific data ● Authors did not account for neonatal morbidity and mortality due to cervical lesions |
GNV with 9vHPV was cost-effective |
| Belgium | Simoens 202123 | 11- to 12-year-old males and females | 9vHPV GNV | 2vHPV FOV | Dynamic transmission | EUR, 2017 | Y | Lifelong | F: 90% M: 90% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 1.5%/3% | Discount rate | ● The model did not assess possible changes to cervical cancer screening methods over the course of the 100 years ● The model also did not assess indirect costs, the impact on fertility, as well as neonatal morbidity and mortality due to cervical lesions ● Currently, disease transmission among populations at high risk, such as MSM and HIV populations, is not included in the model, which may result in underestimating the added benefit of male vaccination compared with an FOV strategy. ● The model may overestimate herd immunity, or the protective effects of vaccination at a population level, even among those who were not vaccinated. No migration into Belgium was assumed, and the model is not able to account for the historical mixed schedule (i.e., 2vHPV and 4vHPV in different regions) ● The model incorporated the impact of the vaccine on HPV 31/33/45/52/58 types that cause cervical and anal cancer only and not HPV-related diseases such as vulvar, vaginal, and head and neck cancers |
GNV with 9vHPV was cost-effective |
| France | Majed 202126 | 11- to 14-year-old males and females | 9vHPV GNV | 9vHPV FOV | Dynamic transmission | EUR, 2018 | Y | Lifelong | F: 26.2% M: 6.2% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 4%/4% | Price, discount rate, duration of protection | ● It was assumed that all model inputs would remain constant over the time horizon. This is a strong assumption as VCR and screening rates would probably change over time. Because incidences of CIN1 and CIN2/3 were not part of the calibration targets, the current analysis underestimates incidence of CIN1- CIN2/3. Consequently, this approach would result in an underestimate of the impact of vaccination. ● The results may underestimate the benefits of the vaccination because indirect effects (neonatal morbidity and mortality due to cervical lesions) and indirect costs (productivity losses) of HPV-related diseases have not been considered. Tthe societal perspective was not incorporated in the disease, mortality, and vaccine related costs. Consequently, the results shown here likely underestimate the true value of the 9-valent vaccine as it would be expected to lead to even higher cost avoided when incorporating relevant indirect costs from the societal perspective ● The model required some parameters that could not be found from French-specific publication(s), which may limit the validity of the results ● The model assumes that the death rate for undiagnosed cancer (all stages) is the same as that of diagnosed cancers. The QALYs gained due to deaths avoided includes deaths due to both diagnosed and undiagnosed cancer and may overestimate the benefit of vaccination |
GNV with 9vHPV was cost-effective |
| Italy | Haeussler 201549 | 12-year-old males and females | 4vHPV GNV | No vaccination/4vHPV FOV | Dynamic Bayesian Markov | EUR | Y | Lifelong | F: 90% M: 90% |
AC, CC, H&NC/OPC, GWs, PC, VaC, VuC | 3%/3% | Price, discount rate, duration of protection, non-CC-related cases, efficacy, cross-protection, sexual activity, frequency of CCS | NR | GNV with 9vHPV was cost-effective |
| Italy | Mennini 201720 | 12-year-old males and females | 9vHPV GNV | 2vHPV/4vHPV FOV/GNV | Deterministic, dynamic, ODE-based SIRS transmission | EUR, 2014 | Y | Lifelong | F: 71.1% M: 71.1% |
AC, CC, CIN1, CIN2+, GWs, VaC, VuC | 3%/3% | Discount rate | ● One limitation of this analysis is that the model involved numerous parameters, and not all relevant parameters could be found from Italian- specific publication(s), which may limit the validity of the results. However, non-Italian-specific values have been validated by experts and usually refer to population-independent parameters ● To simplify the calculations in the model, identical attribution to each of the 5 additional 9vHPV types—31, 33, 45, 52, 58—was included ● Finally, probabilistic sensitivity analysis was not performed because the interface of the model does not allow to quickly modify and evaluate several scenarios. However, the deterministic sensitivity analyses conducted to address the uncertainty showed that the conclusions of our analysis are robust |
GNV with 9vHPV was cost-effective |
| Italy | Barbieri 202343 | 12-year-old males and females | 9vHPV GNV | No vaccination/Current vaccination | Static cohort | EUR, 2020 | N | Lifelong | F: 42% to 95% M: 32% to 95% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, PC, VaC, VuC | 3%/3% | Coverage | ● The HPV vaccination, addressed to an adolescent population, and thus having a long life expectancy, prevents potentially very serious diseases with consequent high morbidity and mortality, and shows a higher return on investment compared with vaccinations addressed to an older population ● The analysis performed is highly conservative ● There is uncertainty about some of the data used in the model; this has an important impact on the results of the analysis. ● A limitation of the analysis is the choice of static models that consider only a fixed cohort of individuals for each model. Dynamic models would have given the chance to estimate the impact of the reduction in disease incidence for future cohorts (for HPV in particular) and the benefits in terms of herd immunity for the population at large (for HPV and influenza). The use of such models goes beyond the scope of our analysis but is more common in cost-effectiveness models. |
GNV with 9vHPV was cost-effective |
| Italy | Cherif 202352 | Males and females | GNV (adolescents +young adults+ CU) | GNV adolescents only | Age-structured HPV infection and disease-progression | EUR | - | 5 to 10 years | - | - | - | - | NR | AA+YA (all durations), AA+YA+SC (5-, 10-year duration), AA+YA+MAW (10-year duration) are relatively more cost-effective compared to AA |
| North America | ||||||||||||||
| Canada | Laprise 201455 | 12-year-old males and females | 2-/3-dose 4vHPV FOV/GNV | No vaccination/2-dose FOV 4vHPV | Dynamic transmission | CAN$, 2010 | N | 10 years to Lifelong | F: 80% M: - |
AC, CC, CIN2+, H&NC/OPC, GWs, PC, VaC, VuC | 3%/3% | Dosing schedule, duration of protection, price, herd immunity, disease burden of MSM | ● A limitation of our analysis is the validity of data on the proportion of MSM in the population and the burden of disease within this population. However, even when the proportion of MSM was assumed to be high (7% vs. 3% in the base case), vaccinating boys with 2 doses remained dominated by 3-dose girls-only vaccination ● The model assumes no herd protection from girls-only vaccination to MSM. Herd protection to MSM is only included in scenarios with male vaccination, potentially overestimating the impact of including boys in vaccination programs |
Two-dose GNV was not cost-effective unless the cost/dose for males was substantially lower than the cost for females |
| USA | Laprise 201656 | 9- to 14-year-old males and females | 2-dose 9vHPV FOV/GNV | No vaccination/3-dose 9vHPV FOV/GNV | Dynamic transmission | USD, 2013 | N | 10 years to Lifelong | - | AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, PC, VaC, VuC | - | Duration of protection | ● First, the duration of protection conferred by 3 or 2 doses of HPV vaccines is still unclear. However, data suggest that the duration of protection after 3 doses of vaccine will be long-lasting, with no evidence of loss of vaccine protection through 8–10 years of follow-up ● Furthermore, it is unknown whether the duration of protection conferred by 2 doses will be like that of 3 doses. However, the 9-valent trial found that antibody titers at one month after the last dose were noninferior and actually higher in the adolescents who received 2 doses separated by 6 or 12 months, compared with the young adult women who received the standard 3-dose schedule |
Substantial healthcare cost-saving if 2-dose 9-vHPV provides at least 20 years of protection |
| USA | Chesson 201162 | 12-year-old males and females | 4vHPV FOV/GNV | No vaccination/4vHPV FOV | Transmission | USD, 2008 | Y | Lifelong | F: 20% to 75% M: 20% to 75% |
AC, CC, H&NC/OPC, PC, VaC, VuC | - | Price, coverage, efficacy | ● One key limitation that might have led to an underestimation of the cost per QALY gained by expanding male vaccination recommendations is that our model does not stratify by risk behavior. Although the incidence rates we applied for HPV-associated health outcomes in males are population-level estimates that include special populations such as MSM, the model does not specifically account for these special populations ● Our comparison strategy was defined as vaccination of females through age 26 years and males through age 21 years. This comparison strategy was based on the current vaccination approach but does not precisely match the current ACIP recommendations for HPV vaccine for older males ● Our model is not well-suited for accounting for the potential costs and benefits of those who initiate but do not complete the vaccine series |
GNV with 4vHPV was cost-effective if female coverage was low and all potential health benefits of HPV vaccination were included |
| USA | Kim 200964 | 12-year-old males and females | 4vHPV/2vHPV GNV | FOV | Disease simulation | USD, 2006 | Y | Lifelong | F: 75% M: 75% |
AC, CC, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | Non-CC related cases, price, coverage, efficacy, waning immunity | ● Firstly, assumptions about sexual behavior were simplified on the basis of large population surveys; however, variables of the dynamic model were calibrated to fit age-specific prevalence of HPV in the population, such that the implications of our assumptions on sexual mixing were consistent with empirical data ● Secondly, individuals in the population are likely to benefit differentially from the vaccine. A limitation of our analysis is that we only represented heterosexual partnerships and therefore did not reflect HPV transmission among men who have sex with men, who face a high risk of anal cancer and may realize a greater benefit from HPV vaccination. Such an analysis would require a more comprehensive model that includes a fuller range of sexual behaviors, which we acknowledge as an important priority for future work ● Data on incidence, mortality, and quality of life associated with HPV-related cancers other than cervical cancer are also limited. We used multiple models to leverage the different levels of data available for each health condition, yet inconsistencies between model types and complexities associated with model linkage should be further explored ● Fourthly, data on vaccine efficacy are reported primarily for females and include outcomes related only to HPV infections, precancerous lesions, and genital warts. Longer-term data on vaccine properties of both the bivalent and quadrivalent vaccines will be important to incorporate when available, to provide more accurate estimates of their expected benefits and costs |
4vHPV GNV was not cost-effective |
| USA | Ortiz 201761 | 11- to 15-year-old males and females | 4vHPV GNV (high coverage) | 4vHPV GNV (low coverage) | Dynamic transmission | USD | Y | Lifelong | F: 34% to 80% M: 13% to 64% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | - | Coverage | ● Among publication(s) limitations is the exclusion of health benefits and cost offsets associated with other HPV-related-diseases which may be a consequence of HPV 6, 11, 16 and 18 infections, whose inclusion may show an improvement on HPV4 cost-effectiveness ● Also, only direct medical costs were included in the analysis; HPV-associated labor productivity loss was not included, which represented for the US an estimate of $1 billion in cervical cancer ● Another limitation of the publication(s) is that data on the age-specific incidences of genital warts are under-reported in Puerto Rico, leading to inaccuracies in the model estimations. We therefore calibrated the model based on the annual age-specific incidences of GWs in the US ● In addition, data pertaining to the costs of follow-up care for incident episodes of HPV-related disease, including genital warts, were not publicly available. Therefore, these costs were estimated based on claims analysis from a private health insurance company (using ICD 9 and CPT codes). More accurate estimations of these costs represent an area for future research |
GNV with 4vHPV with increased coverage was cost-saving |
| USA | Elbasha 200858 | 12- to 24-year-old males and females | 4vHPV FOV/GNV+ CCS ± CU for females/males | CCS | Nonlinear, deterministic, age-structured, mathematical | USD, 2005 | Y | Lifelong | F: 70% M: 70% |
CC, CIN1, CIN2+ | - | Duration of protection, price, coverage, quality of life | ● First, more relevant data on the natural history of HPV infection and disease are needed. For example, epidemiological publication(s) of disease transmission are necessary to estimate the transmission probability per sexual contact. Also, given the influence utility data have on the cost-effectiveness ratios, more publication(s) are needed to collect health utility data for the HPV disease states considered in this model ● Second, we modeled only 2 HPV types and their associated diseases and assumed that HPV types have independent natural histories with no interaction (whether synergistic or antagonistic) among them ● Third, the model assumed that the sexually active population has equal access to healthcare, be it vaccination, screening, or treatment. However, this may not be realistic and may overestimate the benefits of vaccination if women who have limited access to screening are also less likely to get vaccinated ● Fourth, the current version of the model focuses on heterosexual transmission of HPV. It may be desirable to incorporate transmission between homosexuals and heterosexuals in a single model ● Fifth, the scope of the model has been limited to cervical cancer, CIN, and genital warts. HPV infection has also been associated with cancers of the anus, penis, vagina, vulva, and head and neck, as well as recurrent respiratory papillomatosis |
GNV with 4vHPV is cost-effective if vaccination was done before 12 years and included CU with 12-24 years |
| USA | Brisson 201631 | 13- to 17-year-old males and females | 4vHPV GNV/9vHPV for females and 4vHPV for males/9vHPV GNV | No vaccination/4vHPV GNV/9vHPV for females and 4vHPV for males | Multiple individual-based transmission-dynamic | USD, 2010 | Y | Lifelong | F: 25% to 62% M: 25% to 62% |
AC, CC, CIN2+, H&NC/OPC, PC, VaC, VuC | 3%/3% | Price, coverage | ● Firstly, we assumed equal 9-valent vaccine efficacy for girls and boys based on immunogenicity bridging data. However, we predict that vaccinating boys with the 9-valent has very little incremental benefit; thus assumptions about vaccine efficacy among boys are unlikely to impact our overall conclusions ● Secondly, the duration of 4- and 9-valent vaccine efficacy and future HPV vaccination coverage remain unknown. In our base case, we assumed that duration of protection would be lifelong and coverage would plateau among both girls and boys based on current vaccine uptake rates. However, our results clearly show that our findings are insensitive to vaccine duration and that even when vaccination coverage is high, switching to a 9-valent gender-neutral vaccination remained very cost-effective ● Authors did not examine the cost-effectiveness of the 9-valent vaccine relative to the 2-valent, as the 4-valent is used in the United States and most HIC ● Model did not examine scenarios where the 9vHPV would allow more aggressive changes in screening, further reducing future costs |
GNV with 9vHPV was cost-saving if the additional cost/dose of 9vHPV was <$13. GNV with 9vHPV is very cost-effective if vaccine coverage was high |
| USA | Choi 202260 | 9-year-old males and females | GNV (high coverage) | GNV (low coverage) | Decision analytic Markov cohort simulation | USD, 2020 | Y | - | F: 53.7% to 80% M: 48.7% to 80% |
OPC | 3%/3% | Coverage | ● First, only the sex and age dependence were considered without incorporating other potential factors affecting vaccination uptake rates, risk of oral HPV infection and OPC, such as socioeconomic or demographic factors. The examination of health benefits in each subpopulation, however, is more nuanced due to differences in HPV infection, vaccination initiation and completion, and OPC incidence rates, and the likelihood of catching infection and adherence till recommended doses also vary by economic status, education, and general willingness and outlook towards vaccination. A thorough incorporation of important determinants and individualized simulations remains an area for future research ● The expected cost of HPV vaccination promotion efforts was not incorporated in our model; thus, our results of cost-effectiveness analysis, particularly for males, would be dependent on the cost needed to increase the coverage rate. The results of our analysis could be used as a guideline to support a decision on budget allocation for the HPV vaccination promotion strategies ● Because a Markov-cohort model was used in this analysis, individual-level transmission, which is common in infectious disease models, was not specifically modeled. The calibrated infection and progression rates were assumed to be constant by age and sex and only serve as proxy for more detailed individual level transmissions |
GNV with high coverage was cost-effective |
| USA | Laprise 202024 | 11- to 45-year-old males and females | 9vHPV GNV up to 26 to 45 years | 9vHPV GNV aged 11 to 26 years | Dynamic transmission | USD, 2018 | Y | Lifelong | F: 2.6% M: 1.9% |
AC, CC, CIN2+, H&NC/OPC, GWs, PC, VaC, VuC | 3%/3% | Coverage, efficacy, natural immunity after infection, progression rates after infection | ● First, the long-term herd effects on mid-adult women and men from vaccinating younger cohorts remain uncertain. If our model overestimates the herd effects of the current program, vaccinating mid-adult women and men might produce greater benefits and lower ICERs than predicted. However, our model reproduces short-term postvaccination herd effects. Furthermore, we examined a scenario assuming no herd effects from teens and young adults and found that even under this extreme scenario, vaccinating 80% of women and men at age 30 years would cost $184,000 per QALY gained. ● Second, considerable uncertainty also exists about the level of natural immunity after infection and the rate of progression from infection to lesions. When parameter sets with the lowest natural immunity levels and fastest progression from infection to CIN1/2/3 were used, vaccinating mid-adults through age 30 years (vs. current vaccination) produced greater benefits and lower ICERs than predictions from all parameter sets ● Third, the distribution of ages at which cancer-causing infections are acquired is unknown. If causal infections occur at a later age than forecasted by our model, mid-adult vaccination might yield greater benefits and lower ICERs than predicted ● More than half of new cervical cancer cases in the United States occur among under- or never-screened women |
9vHPV GNV was cost-saving when females aged 11 to 26 and males aged 11 to 21 years were considered |
| USA | Elbasha 201057 | 9- to 26-year-old males and females | 4vHPV GNV | 4vHPV FOV | Transmission | USD, 2008 | Y | 32 years | F: 90% M: - |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | Price, efficacy, cross-protection, costs of non-CC cases | ● First, relevant data on the natural history of site- and type-specific HPV infection and disease are lacking in some areas. For some of the non-cervical HPV diseases we had to infer some of these parameters through calibration techniques. Also, more data are needed on health utilities of HPV disease states. ● Second, we created separate and independent models for each HPV-type/disease combination. This amounted to assuming that HPV types have independent natural histories with no interaction among them. If there are significant competing risks (e.g., cross-immunity between HPV types or effects of treatment on prevalence of other types and associated disease), our estimates of the cost-effectiveness ratios of vaccination programs may be inaccurate ● Third, the current version of the model focused on heterosexual transmission of HPV and did not incorporate transmission between homosexuals and heterosexuals, or men who have sex with men. Fourth, the efficacy of HPV4 has not yet been clinically demonstrated in anal, penile, head/neck or RRP disease. If our projections regarding the impact of vaccination on these diseases differ from the true clinical benefit among these diseases, our cost-effectiveness results could change ● Finally, probabilistic sensitivity analysis was limited to inputs related to vaccine properties and uptake, cost, and quality of life weights, and did not include all demographic, behavioral, screening, clinical, and other natural history parameters |
GNV with 4vHPV including boys and men aged 9 to 26 years was cost-effective |
| USA | Chesson 201659 | Males and females | 9vHPV to females (aged 13 to 18 years) to previously completed 4vHPV FOV | 9vHPV GNV | Dynamic transmission | USD, 2013 | Y | Lifelong | F: 46% M: 25% to 29% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, PC, VaC, VuC | 3%/3% | Quality of life | NR | GNV with 9vHPV was cost-saving. Further additional 9VHPV to the population who completed the vaccine series was not cost-effective |
| USA | Daniels 202121 | 13- to 45-year-old males and females | 9vHPV GNV + CU 13-45 years | 9vHPV GNV + CU (13–26-year-old females and 13–21-year-old males) | Non-linear, deterministic, mathematical model of the transmission dynamics | USD, 2018 | Y | Lifelong | F: 22.8% to 72.7% M: 0 to 58.6% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | Coverage, health utility, discount | ● HPV-related cancers affect women and men of working age and therefore affect their productivity. Authors did not consider the indirect costs related to productivity losses ● We assumed that sexual behavior among adults has not changed significantly since 2002. In addition, we calculate risk of HPV transmissible sexual contacts using the annual number of sexual partners for each age group. ● The approach may overestimate the risk of HPV transmission, especially among older populations. ● The model does not account for recent updates to pre-vaccine era estimates of cervical cancer and other disease incidences, nor does the model account for changes in background cancer incidence, e.g., cervical cancer incidence has been falling since 2005 and oropharyngeal cancer incidence has increased |
Expanded CU of males and females aged 9–45 years was considered cost-effective |
| USA | Chesson 201818 | 12- to 26-year-old females and 12- to 26-years-old males | 9vHPV GNV + CU male 12 - 26 years | 9vHPV GNV + CU (12–26-year-old females and 12–21-year-old males) | Deterministic, dynamic, population-based | USD, 2016 | N | Lifelong | F: 2.6% to 29.5% M: 1.9% to 24.9% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | Natural immunity after infection | ● The model does not stratify by risk behavior; this might have led to an underestimation of the cost per QALY gained by expanding male vaccination ● Although the incidence rates we applied for HPV-associated health outcomes in males are population-level estimates that include special populations such as MSM, our model does not specifically account for these special populations ● The comparison strategy was defined as vaccination of females through age 26 years and males through age 21 years. This comparison strategy was based on the current vaccination approach but does not precisely match the current ACIP recommendations for HPV vaccine for older males |
GNV with 9vHPV including an expanded male population aged 26 was not favorable |
| USA | Chesson 202063 | 27- to 45-year-old males and males | 9vHPV GNV + CU 12-45 years | 9vHPV GNV + CU (12–26-year-old females and 12–21-year-old males) | Deterministic, dynamic, mathematical | USD, 2018 | N | Lifelong | F: 2.6% M: 1.9% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | HPV acquisition by age | ● The model does not stratify beyond age and sex and thus does not account for heterogeneity in risk behavior or for special populations such MSM, who are at higher risk than other men for HPV infections and related diseases ● The model assumes lifelong duration of vaccine protection and is unable to examine scenarios of waning vaccine protection ● The model also assumes constant cancer incidence rates in the absence of vaccination ● Cost-effectiveness estimates were more favorable for HPV vaccination in general (including mid-adult vaccination) when we assumed recent trends in cancer incidence would continue ● The model cannot specifically account for the possibility that vaccination could provide protection against re-infection |
GNV with 9vHPV of mid-adults is much less cost-effective than 9vHPV of adolescents and young adults |
| USA | Chesson 201619 | 12- to 26-year-old females and 12- to 21-year-old males | 9vHPV GNV + CU | 4vHPV GNV + CU | Deterministic, dynamic, population-based | USD, 2013 | N | Lifelong | F: 0.8% - 20.6% M: 0.3% - 5.3% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, RRP, PC, VaC, VuC | 3%/3% | - | ● The model uses discrete, 1-year time steps (rather than a continuous approach as in more complex models), which might cause an underestimation of the speed and degree to which HPV vaccination affects HPV transmission dynamics in the population. ● The model does not explicitly account for cervical cancer screening and therefore cannot examine the impact of future changes in cervical cancer screening. Instead, our model approximates the long-term costs and benefits of HPV vaccination under the assumption that the probability of detection through screening remains constant over the duration of the HPV vaccine program and that the number of cervical cancer cases would remain constant over time in the absence of vaccination ● The model does not explicitly account for the progression from HPV infection to disease. Instead, reductions in HPV-attributable outcomes are approximated based on the reduction in the acquisition of the HPV vaccine types over time ● Authors assumed that all those who initiated the vaccine series would receive all 3 doses and that vaccine duration of protection would be lifelong ● The analysis did not include potential adverse effects of vaccination (e.g., temporary pain at injection site) or the potential for HPV type replacement. Our model might underestimate the benefits of 9vHPV if there is type replacement after introduction of 4vHPV, although current data do not indicate the occurrence of type replacement |
GNV with 9vHPV was cost-saving |
| USA | Kim 202128 | 30- to 45-year-old males and females | 9vHPV GNV | 9vHPV of women up to 26 years of age and men up to 21 years of age | Dynamic | USD, 2018 | Y | Lifelong | F: 2.6% to 29.5% M: 1.9% to 24.9% |
AC, CC, CIN1, CIN2+, H&NC/OPC, GWs, PC, VaC, VuC | 3%/3% | Natural immunity after infection, price | ● Authors erred in the direction of making assumptions that were favorable to increasing the age of vaccination, including assuming no delay between the reduction in HPV infections from vaccination and the reduction in genital warts Authors assumed that there could be an impact of HPV vaccination on incidence of noncervical cancers as early as 5 years after vaccination. This minimum lag time may be longer.) Authors did not take into consideration potential changes in the future burden of the noncervical cancers (other than through vaccine impact) and instead assumed the current underlying age-specific incidence and mortality rates remained constant over time To the extent that the incidence rates of these cancers are rising (e.g., oropharyngeal cancers in men), model may be underestimating the overall benefit of HPV vaccination |
GNV with 9vHPV for adult women and men aged 30 to 45 years is unlikely to represent good value for money |
| USA | Durham 201629 | 11- to ≥77-year-old males and females | 9vHPV GNV | 4vHPV/2vHPV GNV | Age-structured compartmental | USD, 2016 | Y | Lifelong | F: 20% to 57% M: 9% to 43% |
CC | 3%/3% | - | ● All HPV models are limited by epidemiological and clinical uncertainty, particularly with respect to HPV and vaccine-induced immunity ● Authors assumed no interactions among HPV types. ● The model does not differentiate between the sexual behavior and vaccination decision-making of individuals who move to another state and individuals who do not leave their home state |
GNV with 9vHPV was cost-effective |
Abbreviations: 4vHPV, quadrivalent vaccine; £, pounds sterling; AA+YA+MAW+SC, adolescent+young adult+mid-adult+opportunistic single cohorts for females aged 30, 35, and 40 years; AC, anal cancer; CAN$, Canadian dollars; CC, cervical cancer; CCS, cervical cancer screening; CIN, cervical intraepithelial neoplasia; CU, catch-up vaccination; EUR, euros; FOV, female-only vaccination; GDP, gross domestic product; GNV, gender-neutral vaccination; GWs, genital warts; H&NC, head and neck cancer; HKD, Hong Kong dollars; HPV, human papilloma virus; ICER, incremental cost effectiveness ratio; INT$, international dollar; KRW, Korean won; MSM, men who have sex with men; NOK, Norwegian kroner; NZ$, New Zealand dollars; OPC, oropharyngeal cancer; PC, penile cancer; QALY, quality-adjusted life-years; RCT, randomized controlled trial; RRP, recurrent respiratory papillomatosis; SEK, Swedish krona; SGD, Singapore dollars; SIRS, susceptible-infected-recovered susceptible model; USD, US dollars; VaC, vaginal cancer; VuC, vulvar cancer.
Comparators and publication(s) questions
Twenty-nine publications evaluated the cost-effectiveness of 9vHPV compared to bivalent HPV vaccination, quadrivalent HPV vaccination, or no vaccination.17–45
Country and funding
Among included publications, the majority (47/53) were conducted in high-income countries, including countries in Asia (Hong Kong [n = 1], Japan [n = 1], South Korea [n = 1], Singapore [n = 3]),34,39,41,44–46 Europe (Austria [n = 2], Belgium [n = 1], Denmark [n = 1], France [n = 1], Germany [n = 1], Greece [n = 1], Ireland [n = 1], Italy [n = 4], Netherlands [n = 1], Norway [n = 2], Spain [n = 1], Sweden [n = 1], United Kingdom [UK; n = 4], multiple European Union [EU] countries [n = 1]),17,20,22,23,25–27,30,32,33,35–38,40,43,47–53 Oceania (New Zealand [n = 1]),54 and North America (Canada [n = 1], United States [US; n = 16]).18–20,24,28,29,31,55–64 Five publication(s) were conducted in upper-middle-income countries (Brazil, Colombia, El Salvador, Türkiye),42,65–68 and one publication(s) was conducted in a lower-middle-income country (Vietnam), although the publication(s) was restricted to the southern region of the country.69
Approximately 35.8% (19/53) of publications were funded by vaccine manufacturers (e.g., Merck, Sharp & Dohme; Sanofi Pasteur MSD),17,20–23,25,26,30,36–38,41,44,46–49,57,61 and 30.2% of publication(s) (16/53) were funded by not-for profit funders.24,27–29,31,33,40,50,53–56,59,60,64,69 The remaining 18 publication(s) did not specify their funding sources.18,19,32,34,35,39,42,43,45,51,52,58,62,63,65–68
Patient age
Five publications assessed pre-adolescent (<10 years of age) populations, 28 assessed adolescent (10–17 years of age) populations, and 20 considered mixed populations (i.e., pre-adolescent, adolescent, and adult populations).
Type of economic analysis
Thirty-four studies17–19,23–27,30,33–42,44,45,48–52,56,57,59,60,62–64,68 were cost-effectiveness analyses (CEAs), while 3 publication(s)40,47,55 were cost-utility analyses (CUAs). Sixteen publication(s)20–22,28,29,31,32,46,53,54,58,61,65–67,69 performed both cost-effectiveness and cost-utility analyses.
Model type
The majority of the included publication(s) used a single dynamic transmission model (n = 38). Nine publication(s) had static models,18,39,43,49,54,59,60,62,63 of which seven publication(s)18,49,54,59,60,62,63 included some method for accounting for herd immunity. Among publication(s) that used a single dynamic transmission model most were deterministic (n = 30) and the remainder (n = 8)24,31,48,50,55,56,64,69 were stochastic (all of which were agent-based models). Two publication(s) included analyses from multiple models.50,64 One did not provide enough information to classify its methods.32
Model perspective
Seventeen publication(s)18,20,21,24,28,33,37,39,40,48,51,53,54,60,61,63,68 reported their analyses from a healthcare provider perspective, and 14 publication(s)17,22,23,25,26,30,34,36,38,41,42,44,47,55 from a payer perspective. Eleven publication(s)19,29,31,43,46,50,56,59,62,64,69 reported analyses from a societal perspective, while 1 publication(s)34 reported from multiple perspectives, including the United Kingdom (UK) National Health Service (NHS) and personal social services perspectives. The remaining 10 publication(s)32,35,45,49,52,57,58,65–67 did not specify a modeling perspective.
Time horizon and discount rates
Regarding time horizon, 35 publication(s) projected outcomes over a 100-year time frame, while 8 publication(s) reported a lifetime time horizon,20,33,34,43,50,53,64,69 and 7 publication(s) reported time frames between 35 to 85 years.29,31,40,48,49,55,60 One publication(s) assessed the cost-effectiveness of gender-neutral adult HPV vaccination in Italy over 3-, 5-, and 10-year time frames.52 The remaining 2 publication(s) did not specify the time horizon.32,67
Most publication(s) (33/53) applied discount rates of 3% to costs.17–22,24,25,29,31,33–35,39,42–44,46–49,51,53–57,59,60,64,68–70 One publication(s) applied 3.5%,27 2 publication(s) applied 4%,26,50 and 2 applied 5%.65,66 Among those reporting discount rates less than 3%, 2 publication(s) reported 1.5%.23,38 The discount rate was differential (between 1% and 4%) in 4 publication(s).36,37,40,45 One publication(s) did not specify the discount rate used in its economic evaluation.62
Sensitivity analyses
Among the 53 included publication(s), 31 conducted sensitivity analyses, of which 21 were one-way sensitivity analyses18–24,26,28,30,31,37,39,41,44,50,59,60,62,63,69 and 5 publication(s) were multi-way sensitivity analyses.48,50,55,62,63
Diseases covered
Cervical cancer was covered in 50 publication(s), while the non-cervical cancers reported in included publications were vulvar (n = 43), vaginal (n = 43), anal (n = 44), penile (n = 40), head and neck/oropharyngeal (n = 43), and recurrent respiratory papillomatosis (RRP; n = 25). Mild cervical intraepithelial neoplasia (CIN 1) and moderate to severe cervical intraepithelial neoplasia or carcinoma in situ (CIN 2+) were covered in 37 publication(s), while genital warts were considered in 42 publication(s).
Duration of vaccine protection
Approximately 58% (31/53) of publication(s) assumed lifelong vaccine protection,17,18,20–26,28,30,31,37,40,43–46,48–51,53,55,58,59,61–63,68,69 while 3 publication(s) assumed a duration of 35–25 years,40,54,55 4 publication(s) assumed a shorter duration of 20 years or less,27,40,54,55 2 publication(s) varied their assumptions between lifetime for vaccine type – specific genotypes and 10 years for non-vaccine type – specific genotypes,36,56 and 13 publication(s) did not specify duration of vaccine protection.32–35,38,39,41,42,52,53,60,65,67
Cross-protection, herd immunity, and disease transmission
Cross-protection of various HPV types was considered in the models of 11 publications.17,27,31,33,34,36,38,42,43,49,55,59,64 Most analyses included herd immunity (n = 36), assuming that protection of females from genital warts through vaccination also protects their male partners against warts and vice versa. The majority of the model analyses (n = 49) assumed heterosexual transmission of HPV disease and did not incorporate other scenarios, while 4 publication(s) considered homosexual transmission in their analyses.39,51,54,55 Also, no included publication(s) assumed any effect from vaccination on the natural course of HPV infection present at the time of vaccination. Most publication(s) (29/53) also incorporated cervical cancer screening.17,20–26,31,36,37,40,41,44,46–50,55,57,61–66,68,69
Quality assessment
The HPV FRAME checklist and CHEERS checklists were used to assess the extent of the standards for reporting followed by the included publication(s). Only full-text articles (n = 43) were critically evaluated for quality assessment. In total 41 articles included adolescents, 9 included adults, and 4 included the men who have sex with men (MSM) population. Twenty-two publications included cervical cancer screening in their strategy. Across publications that reported the details of the target population (n = 45), almost all the publication(s) provided the details of the population either by age, sex, or both. Sexual behavior parameters, including age-specific sexual behavior or lifetime number of partners and age at sexual debut, were reported in 32 publication(s). The model time horizon was reported in all 43 journal articles. Calibration and validation used in the model analyses were described in 50% of the publication(s). ICERs, sensitivity analyses, vaccine uptake, and vaccine efficacy were described in approximately 40 publication(s). Vaccine cross-protection was reported in 14 publication(s) reporting on adolescents and 3 publication(s) with adult populations. Among publication(s) with MSM populations (n = 4), all publication(s) reported vaccine coverage.
publication(s) results
Vaccination of adolescent males and females evaluating 4vHPV
In total, 17 publication(s) reported on vaccination with 4vHPV of adolescent males and females, of which 14 publication(s) concluded 4vHPV was likely to be cost-effective. Among upper-middle-income countries (e.g., Brazil, Colombia, and El Salvador),65–68 vaccination with 4vHPV was a cost-saving strategy when high coverage rates (e.g., 50% to 80% in both females and males) were considered in comparison to low coverage rates (e.g., 35% to 85% in females and 10% to 50% in males). However, the coverage for males and females differed across countries: 80% in Denmark,48 the US,48,60 and Sweden,51 65% in Austria,47 and 71% in Norway50 and the US.50 In a cost-effectiveness analysis on the impact of HPV coverage on HPV-associated oropharyngeal cancer using a hypothetical cohort of 9-year-old boys and girls in the US, high vaccine coverage (e.g., 80% in males and females) was considered cost-effective as it led to a substantial reduction in oropharyngeal cancer cases by almost 50% in males60 compared to the status quo (53% in females and 48% in males). In contrast, in a publication(s) on the cost-effectiveness of adding HPV vaccination of 12-year-old males to a female-only vaccination (FOV) program for ages 12–26 years in the US,62 GNV was considered cost-effective when low coverage rates (e.g., 20% and 30%) and all outcomes (e.g., cervical outcomes, other HPV-related cancers, genital warts, and RRP) were considered versus high coverage rates (e.g., 75%). The model did not account for the possibility of female sex partners of vaccinated men being more likely to be vaccinated and have access to cervical cancer screening than the unvaccinated men, which could have overestimated the opportunities of male vaccination to achieve reductions in HPV-related health outcomes in female partners. In Burger et al. (2014),50 which evaluated the cost-effectiveness of expanding HPV vaccination in Norway to include pre-adolescent boys, GNV was cost-effective when there was coverage of 71% for males and females, high vaccine efficacy, and a vaccine price of less than $75 per dose. One Singapore publication(s) on the impact of school-based administration of 4vHPV46 reported GNV with 4vHPV was cost-effective compared to a FOV strategy; however, the ICER differed according to the number of doses, with lower rates with a 2-dose schedule compared to a 3-dose schedule ($22,574 vs $27,837 in 2011 Singaporean dollars, respectively). Results from a publication(s) conducted by Elbasha et al. (2008)22 on vaccinating males age 9–26 years in the US suggested that vaccination of males along with females is cost-effective only when catch-up vaccination of females is added.
In contrast, 3 publication(s) (2 in high-income countries55,64 and 1 in a lower-middle-income country)69 concluded that the introduction of male vaccination with 4vHPV was not cost-effective compared to FOV. The factor that impacted the introduction of GNV was the increased cost of male vaccination.55,69 In southern Vietnam,69 adding males to vaccination programs to limit cervical cancer and genital warts became cost-effective compared to a FOV strategy only when the GAVI price of I$5/dose was applied; however, it yielded a marginal benefit in the reduction of cancer cases compared to vaccinating females across all coverage levels. Another publication(s), by Kim et al. (2009)64 was conducted in the US and explored scenarios in which vaccine efficacy and the inclusion of different cancers (i.e., for women only, for both men and women varied; GNV was not cost-effective in any of the scenarios.
Vaccination of adolescent males and females evaluating 9vHPV
Nineteen of 22 publication(s) concluded that GNV with 9vHPV was likely to be cost-effective compared with current vaccine scenarios. Twenty-one of these 22 publication(s) were conducted in high-income countries, and 1 was conducted in Türkiye, an upper-middle-income country. 9vHPV was considered cost-effective in almost all the European17,20,22,23,26,30,32,35–38,40,43 and the US publication(s).31,56
Vaccine coverage, cost, and discount rate impacted cost-effectiveness. In Boiron et al. (2016),22 which assessed the cost-effectiveness of 9vHPV in a universal vaccination program compared to 4vHPV in Austria, vaccinating 60% of females and 40% of males with 9vHPV was deemed cost-effective compared with the current 4vHPV GNV; the ICER was highly dependent on the cost of 9vHPV, and the strategy was cost-saving when the vaccine price was €113 and was cost-effective when the vaccine price was €153. Similarly, in Brisson et al. (2016),31 switching to 9vHPV for females while maintaining 4vHPV for males and 9vHPV GNV as compared to the current 4vHPV GNV program was found to be cost saving in the US if the additional cost/dose for 9vHPV was less than $13. Two publication(s) noted that 9vHPV vaccination was cost-effective when high vaccine coverage for females was considered (<70% in Ireland32 and 70% in Netherlands.38 Alternatively, even a low coverage rate of 26.2% for females and males with 9vHPV was considered a cost-effective strategy in comparison to GNV in a French cost-effectiveness analysis.26 The model considered additional disease-reduction benefits of the vaccine (e.g., cervical cancer, cervical intraepithelial neoplasia, vaginal cancer, vulvar cancer, anal cancer, genital warts, penile cancer, head and neck cancer, and recurrent respiratory papillomatosis). Further publication(s) conducted in Hong Kong,44 the Netherlands,38 and Italy43 suggested that the addition of catch-up vaccination would provide an additional benefit of averting cervical cancer and genital warts cases and accelerate the elimination of genital warts and RRP cases than 9vHPV GNV without a catch-up scenario. In Largeron et al. (2017),17 the introduction of 9vHPV GNV was considered a cost-effective strategy, and the ICER was sensitive to a decrease in the duration of protection, lowering the discount rates for outcomes and the inclusion of all diseases (e.g., cervical cancer, cervical intraepithelial neoplasia, vaginal cancer, vulvar cancer, anal cancer, genital warts, penile cancer, head and neck cancer, and RRP). Further, the dose of 9vHPV impacted the results. In Laprise (2016),56 conducted in the US, the ICER was in favor of 2 doses of 9vHPV FOV/GNV in comparison to 3-dose 9vHPV FOV/GNV, assuming the 2-dose vaccine provided a vaccine protection of ≥20 years. Daniels et al. (2022)30 reported that adopting a single-dose 9vHPV in the UK was not a cost-effective strategy as it resulted in an increase in HPV-related cancer cases in both males and females compared to a 2-dose policy. However, in Song et al. (2024),40 single-dose 9vHPV was considered a cost-effective strategy compared to a 2-dose vaccine. The results were dependent on the vaccine coverage, duration of protection, and cost of the single dose. The publication(s) assumed 90% coverage for 10 years.
Three publication(s), all from high-income countries, concluded vaccination with 9vHPV was not cost-effective. The factors that impacted cost-effectiveness were the price of 9vHPV and the consideration of all HPV-related diseases in the model. Wahab et al. (2023)39 reported that decreasing the total cost of 9vHPV to below $300 would make 9vHPV cost-effective; GNV with 2vHPV was a cost-effective strategy in Singapore versus FOV when a discount rate of 1.5% was applied. Two publication(s)25,33 in Spain also reported that 9vHPV GNV was not a cost-effective strategy when compared to 4vHPV/9vHPV FOV. The model analyses did not consider cross-protection and may have underestimated the impact of vaccines.25 The ICERs were considered potentially cost-effective when vaccine protection against head and neck cancer,25 oropharyngeal cancer,25,33 and penile cancer25,33 was considered.
Vaccination of adolescent males and females versus female-only vaccination
Five publication(s) compared GNV versus FOV, with 3 publication(s) concluding that GNV was the more cost-effective strategy. In a publication(s) conducted in Japan,41 GNV was cost-effective where the females received a 9vHPV at 30% coverage along with a catch-up vaccination at a coverage of 15%, while males received a 4vHPV vaccine at a coverage rate of 15%, which averted 15,695 cervical cancer cases and 1,579 cervical cancer deaths in comparison to 9vHPV FOV. Similarly in Europe,53 vaccination of males remained cost-effective at high vaccine uptake rates across multiple countries. Cherif et al. (2023)52 reported that vaccinating both adolescents and young adults and adding up a catch-up vaccination was more cost-effective than vaccinating just adolescents in Italy.
Two publication(s) concluded that GNV was not cost-effective in comparison to FOV. In the UK, considering the high vaccine uptake in females in the national immunization program, ranging from 78% to 88%, the strategy of targeting the 12- and 13-year-old female population and adding males to the vaccination program using any of the vaccines was not cost-effective, as reported in Datta et al. (2019),40 because vaccine coverage and vaccine price increased. Similarly, in a publication(s)54 conducted in New Zealand, results showed that adding males to what had been a FOV program at either the current vaccine coverage rate (56%) or an enhanced rate (73%) was not determined to be s cost-effective strategy. The ICER was sensitive to high vaccine and administration costs.
Gender-neutral vaccination of adult cohorts
Eight publication(s),18,19,21,24,28,29,57,63 all from the US, discussed the introduction of adult vaccination, an extension of current HPV vaccination to the adult population, or an extension of the routine vaccine to include adult catch-up vaccination for both males and females. In 2019, the Advisory Committee on Immunization Practices (ACIP) recommended vaccination through age 26 in females and age 21 in males. This scenario was evaluated in a publication(s) by Chesson et al. (2016),19 where females aged 12 to 26 years and males aged 12 to 21 years received either 4vHPV or 9vHPV, and 9vHPV was deemed a cost-effective strategy as it provided protection from additional HPV types beyond those covered by 4vHPV. Similar findings were reported in Durham et al. (2016).29 However, the upper recommended age of HPV vaccination varied across the publication(s); in Elbasha et al. (2010),57 vaccinating males aged 9 to 26 against all HPV-associated diseases was a cost-effective strategy compared to a FOV strategy for girls and women aged up to 26 years. The ICER was dependent on the efficacy of 2-dose vaccination, vaccine cost, degree and duration of protection against HPV infection, and higher cost of CIN 2/3, genital warts, and regional penile cancer. In contrast, in Chesson et al. (2018),18 expanding male vaccination from 12 through 26 years (ICER: $228,800/quality-adjusted life-year [QALY]) versus vaccination for females aged 12 through 26 years and males aged 12 through 21 years (ICER: 16600/QALY) was not cost-effective, potentially because the model analysis did not consider the protection against re-infection offered by the vaccine and did not include the MSM population.
Further expanding vaccination to 45 years of age for both sexes was not cost-effective compared to the current strategy of vaccinating females aged 12–26 years and males aged 12–21 years (ICER: $653,300/QALY vs $9,200/QALY, respectively) in 1 US publication(s).63 Similarly, Kim et al. (2021)28 noted higher ICERs for expanding vaccination to ages 30, 35, 40, and 45 years in both the Harvard and the Policy-1-cervix model analyses. They also explored the effect of considering only cervical cancer – related outcomes versus all HPV-related outcomes in the analyses. The cost-effectiveness of vaccinating up to 45 years ranged from $484,900 to $1,011,400 per QALY gained. Although the ICER became more favorable when all HPV-related outcomes were considered, it remained too high (i.e., above the $50,000 to $200,000 per QALY gained threshold) to be cost-effective. There was only 1 scenario in which imperfect screening compliance was assumed; in it, vaccinating up to 40 years was cost-effective at a willingness-to-pay threshold of $200,000.28 Alternatively, vaccination of adults of both sexes was considered cost-effective up to 34 years of age, and for women through age 45 years, in 1 US publication(s).21
Key drivers of cost-effectiveness
Key drivers of the cost-effectiveness of GNV identified in the included publications are presented in Figure 2, with the most commonly reported factors summarized below.
Figure 2.
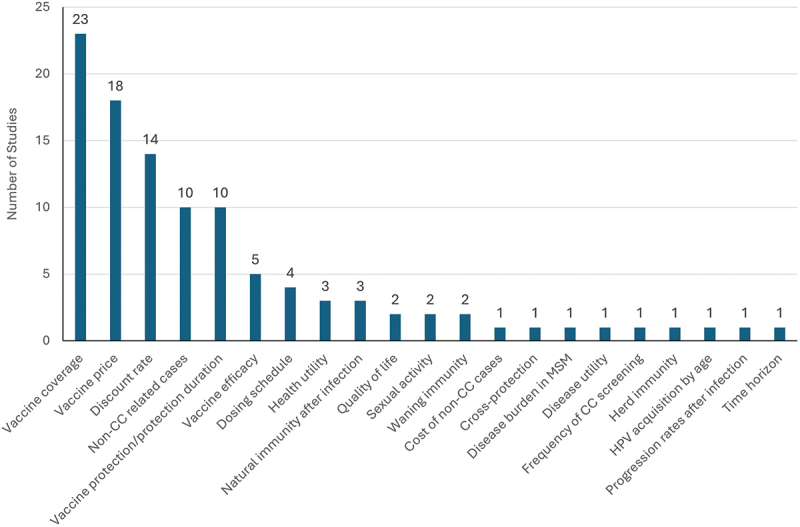
Key drivers of gender-neutral vaccination cost-effectiveness.
Vaccine coverage
In approximately 43% of included publication(s) (n = 23/53), vaccine coverage influenced the cost-effectiveness results. ICERs increased with higher vaccine coverage due to the diminishing marginal benefit of vaccine-induced protection in the population and linearly increasing vaccination costs. Vaccine coverage differed for males and females and ranged between 50% to 80%. Many publications concluded that decreasing coverage rates for girls or females in the analyses improved the ICER, which then became cost-effective for GNV due to the presence of herd immunity.23,25,27,32,53,62,64 In scenarios with low coverage (≤20%), the use of the 4vHPV led to cost savings from a societal perspective. However, low coverage was also associated with fewer prevented cases of cervical cancer.71
Vaccine price
Vaccine price was a key driver of cost-effectiveness in 18 publication(s).22,26,28,30,36,39,40,48–51,55–58,62,64,69 When considering the addition of male vaccination when the price/dose reduces, the ICER improved, making it favorable toward a GNV strategy. publication(s) considering reduced vaccination costs due to reduced dosing schemes or negotiation procedures reached more favorable cost-effectiveness outcomes for the inclusion of males in national HPV immunization programs.40,55,56 The vaccine price ranged widely across the countries, from $5/dose69 in lower-middle-income countries to $75/dose50−1295 Norwegian kroner (NOK)/dose36 in high-income countries. In Australia, GNV was cost-effective when the vaccine price ranged between €113 and €153.22
Discount rates
Cost-effectiveness results were sensitive to discount rates in 14 publication(s).17,20–23,26,27,30,39,40,47–51 The discount rate played an important role when comparing the HPV vaccines with other vaccines or health interventions that return more immediate health impacts. A lower discount rate (e.g., 1.5%) for outcomes yielded more favorable ICERs for GNV vaccination.22,39,47 At high discount rates (e.g., 3%), GNV was not considered cost-effective.39 This sensitivity to discount rates was expected since the benefits of HPV vaccination occur many years after vaccination.
Vaccine protection duration
The duration of vaccine protection was repeatedly noted as a key parameter driving the cost-effectiveness of GNV HPV vaccination programs in 10 publication(s),17,22,26,30,40,49,55–58 as the duration of vaccine protection is uncertain. That is because HPV infections are characterized by a long incubation period between infection and disease onset: infection occurs in an early stage of sexual activity and disease onset many years later. In 1 publication on 9vHPV vaccination in Germany, decreasing the duration of vaccine protection from a lifetime horizon to 20 years improved the ICER results.17 Additionally, the dosing schedule of the vaccine, i.e., 2 doses or 3 doses, was also sensitive to the duration of vaccine protection. For example, one publication comparing 2-dose and 3-dose 9vHPV vaccination in the US concluded that if 2-dose vaccination provided at least 20 years of vaccine protection, a third dose would be very cost-inefficient, while there were benefits of a 3-dose schedule if the 2-dose vaccination schedule provided <20 years of protection.56
Non-cervical cancer and disease cases
Non-cervical cancer and disease cases were reported as key drivers of cost-effectiveness in 10 publication(s).17,26,36,48,49,53,62,64,68,72 Many of the CEA publication(s), although considered GNV, restricted HPV-related outcomes to cervical disease, suggesting that the health impact of male vaccination was underestimated. Three publication(s) concluded GNV to be cost-effective only when all health outcomes of the vaccines were considered.26,62,68 Similarly, 4 publications17,48,49,64 suggested that the addition of all male-related HPV diseases (aged between 12 to 17 years) in the model improves the ICER as compared to adding only the female-related HPV diseases and makes it favorable for expanding FOV to GNV. Furthermore, in many developed countries, the incidence of HPV-related non-cervical cancers has recently increased, particularly for carcinomas of the anus and oropharynx.53,73 Therefore, publication(s) that have also considered the increased patterns in HPV-related disease burden provided results that were more favorable to the inclusion of males in national immunization programs.
Discussion
This SLR summarized publications about HPV GNV cost-effectiveness models and key drivers that influenced cost-effectiveness results. Among publications evaluating HPV vaccination among adolescents with either 4vHPV or 9vHPV, the majority of publication(s) (82.3% and 86.4%, respectively) concluded that GNV was a cost-effective strategy. Among publications comparing GNV among adolescents versus FOV strategies, GNV was mainly cost-effective, although results were dependent on both country-specific disease burden and uptake rates. Among publications on GNV of adults, results on cost-effectiveness were mixed, with variance in the recommended age of HPV vaccination of included publication(s). Key drivers that influenced results among identified cost-effectiveness publications included vaccine coverage, vaccine price, the duration of vaccine protection, and consideration of non-cervical HPV-related cancers and diseases in the model cohorts.
The findings of this systematic review highlight different considerations of HPV GNV economic evaluations. Published publication(s) included in this review were conducted primarily in high-income or upper-middle-income countries; only 1 included publication69 was conducted in a lower-middle-income country. Therefore, there exists a need for further publication(s) from lower-middle-income countries to better understand the potential cost-effectiveness of HPV vaccination in these countries, improve vaccine coverage rates, and address current gaps in immunity.72 Second, most included publication(s) reported that GNV was a cost-effective strategy, although vaccine coverage rates played a significant role in determining cost-effectiveness. While higher coverage rates (i.e., 50% to 80%) for both males and females led to substantial reductions in HPV-related diseases due to herd immunity, the benefit of increasing coverage diminished as vaccination rates approached 100%. The marginal additional health benefits achieved with universal vaccination are therefore not always cost-effective. Naturally, the vaccine coverage rates that are most optimally cost-effective in certain countries are highly dependent on the vaccine price within that country. However, few publication(s) implied that increasing vaccine coverage in females only was likely to be a cost-effective and less costly strategy than GNV.50 In high-income countries like the UK, which had the highest vaccine uptake rates in females (78% to 88%), adding males to the vaccination program was not cost-effective.27
Along with vaccine coverage, vaccine price and discount rates were additional drivers of cost-effectiveness in the included publications. ICERs were highly dependent on the vaccine price, and low vaccine prices were preferred. The vaccine price threshold varied across countries and impacted the vaccine’s cost-effectiveness of the addition of male HPV vaccination. In one lower-middle-income country publication, adding male HPV vaccination to limit cervical cancer and genital warts in southern Vietnam was considered cost-effective only when the Gavi vaccine price was applied.69 High-income countries also were impacted by the high vaccine price, and cost-effectiveness was also dependent on the vaccine price explored. Also, the switch from 2vHPV and 4vHPV to 9vHPV was highly dependent on the cost of the 9vHPV vaccine in the country. In a few publication(s), 9vHPV was not considered cost-effective due to its high vaccine price.39 Additionally, the inclusion of males to current vaccination strategies was not always cost-effective, particularly in high-income countries where vaccine uptake among adolescent girls is already high, due to herd immunity and high vaccine costs. This further emphasizes the benefits of GNV in countries with low coverage, as it may result in improved herd immunity among males as well as additional protection for unvaccinated women. Irrespective of the cohort ages noted in included evaluations (i.e., adolescents, adults, or both), GNV was deemed a cost-effective strategy. However, included publications did not compare cost-effectiveness between age groups, and results should therefore be interpreted with caution.
Reductions in dosing schedules (i.e., from 3-dose to 2-dose GNV vaccination) resulted in cost-effectiveness for GNV vaccination.55,56 However, it is important to note that many people are unable to complete all 3 recommended doses of the HPV vaccine,74 and the impact of vaccine non-adherence was not explored in the included economic evaluations. Therefore, cost-effectiveness results among included estimates may be underestimated. Vaccine protection duration was another impactful driver of cost-effectiveness among included publication(s). However, approximately 58% of publication(s) assumed lifelong vaccine protection in their models, while other published publication(s) have estimated vaccine effectiveness up to 10 years.75 Model results may therefore reflect real-world effectiveness when assuming a shorter duration of vaccine protection.
Finally, the inclusion of non – cervical cancer and disease cases in models impacted cost-effectiveness results. Included models primarily explored the impact on cervical cancer disease reduction and elimination, while publication(s) that also considered the prevention of other HPV-related diseases were more favorable toward GNV strategies. These findings regarding non-cervical cancers were reinforced in the systematic review by Ng et al. (2018) that also explored the cost-effectiveness of GNV programs.12 Additionally, Hidayati et al. (2023) also concluded that HPV vaccination was cost-effective for prevention of non-cervical cancers, including anogenital cancers and head and neck cancers, and recommended expanding HPV vaccination targets to boys, particularly in high-income countries.76 This is particularly important given the increasing incidence of HPV-related diseases among men. In the US, oropharyngeal cancer has surpassed cervical cancer as the most common HPV-related cancer type, and incidence rates for HPV-related diseases are greater among males than females.77 Given the increased screening and treatment of cervical cancers, greater emphasis should be placed on the assessment of non-cervical HPV-related cancers in both men and women unvaccinated against HPV.
This review is subject to several limitations that should be considered in interpreting the findings. First, the findings of this review may be influenced by publication bias since publications with negative or statistically insignificant results are less likely to be published. Second, the cost-effectiveness models employed varied in design, inputs, and assumptions, which limited any quantitative synthesis. The objective of this systematic review was to include publications evaluating 4vHPV and 9vHPV only, which may have excluded articles focusing on 2vHPV. Bivalent HPV vaccination has been proven cost-effective universally versus screening only or no vaccination for prevention of HPV-related cancers. Third, there was the lack of literature from countries listed as low-middle-income, which tend to have greater budget constraints and higher HPV infection rates. Both factors highlight the need for cost-effective strategies regarding GNV HPV programs. Finally, additional factors not explored in this review, beyond economic drivers, may play a role in the implementation of HPV vaccination to current national immunization programs, such as cultural and social nuances, the political landscape, and budget constraints.
Despite these limitations, this review is robust in terms of its systematic methodology, search strategy, and adherence to Centre for Reviews and Dissemination and PRISMA guidelines. The included evidence was not restricted to any specific geographical setting, and publications from all the countries were included to give a comprehensive scenario of HPV vaccine modeling publication(s) across various target vaccination strategies, including girls-only, gender-neutral, and adults. This review has identified the factors that influence the cost-effectiveness of vaccination strategies within included publications and provided an overview of the implication of these determinants on the ICERs, along with possible explanations of such observations, similar to the systematic literature review conducted by Ng et al. (2018)12 However, the earlier review primarily focused on general HPV cost-effectiveness models. Another review published in 2015 summarized publications on the cost-effectiveness of extending HPV vaccination programs to include males in high-income countries,78 concluding that vaccine coverage rate, the inclusion of all HPV-related diseases, and the specific vaccination strategy (i.e., dose schedule, age of vaccination, vaccine program implementation) play a large role in determining the cost-effectiveness of results. Additionally, the publication(s) authors noted that targeting vaccination among the MSM population would be a cost-effective approach to GNV.78 Our review aimed to fill any shortcomings of previously published systematic searches with its focus on more recent literature specific to GNV economic evaluations, its focus on both 4vHPV and 9vHPV vaccines, and its attempt to summarize literature beyond high-income countries.
To enhance the relevance and comparability of future HPV GNV cost-effectiveness publication(s), it is crucial to address several limitations identified in existing models. First, future publication(s) should incorporate differentiated vaccination coverage rates for boys and girls, as well as the potential health benefits of cross-protection offered by the 4vHPV and 9vHPV vaccines. Additionally, models must account for the potential to avert other HPV-related cancers beyond cervical cancer, thereby providing a more comprehensive assessment of vaccination benefits. It is essential to utilize dynamic modeling approaches that reflect real-world variations in HPV transmission, including the inclusion of high-risk populations such as MSM. Furthermore, future research should incorporate societal costs, such as productivity losses, and consider the impact of changes in screening practices over time. To improve generalizability, publication(s) should utilize locally relevant epidemiological data and account for variations in vaccine pricing and healthcare access across different settings. By addressing these factors, future GNV cost-effectiveness publication(s) can yield more accurate and applicable results, facilitating better-informed public health decisions.
Conclusion
Gender-neutral HPV vaccination remains a cost-effective strategy for preventing HPV-related diseases, particularly in regions where non-cervical cancers are prevalent. However, its cost-effectiveness is highly dependent on vaccine coverage (including coverage among girls), vaccine price, duration of vaccine protection, and the inclusion of non-cervical diseases in economic analyses. GNV may not always provide additional value in settings with high female vaccine coverage, but it may benefit areas with lower vaccine uptake or higher disease burden in men. The findings of this systematic review support recommendations for HPV GNV immunization in current country vaccination schedules, the inclusion of HPV vaccination of adolescent boys, and extending the immunization age beyond adolescence for boys and girls. Additional research into the cost-effectiveness of HPV GNV in low-middle-income countries is warranted. Future publication(s) should also incorporate different vaccination coverage rates, the potential to avert other HPV-related cancers beyond cervical cancer, dynamic modeling approaches, the impact of changes in screening practices, and account for variations in vaccine pricing and healthcare access across countries. The ongoing development of cost-effective models, combined with real-world vaccine effectiveness data, will be critical to guiding future vaccination policies globally.
Supplementary Material
Biographies
Marisa Felsher is a harm reduction researcher interested in designing and evaluating social network interventions that increase marginalized populations’ access to HIV prevention strategies. She utilizes mixed methods and community-engaged research approaches, with the goal of translating research findings into health policy and practice. Marisa received an MPH from Columbia University Mailman School of Public health and a PhD from Drexel University Dornsife School of Public Health. She is currently a Stratety and Business lead at Merck.
Marcie Fisher-Borne is a Principal Scientist in the HPV Outcomes Research Unit of Merck. Her expertise includes HPV vaccination implementation science, evidence-based interventions to accelerate HPV vaccination uptake and health systems interventions that improve access. She has a PhD in Social Intervention research from UNC Chapel Hill as well as a masters of public health with a concentration in health behavior.
Nita Santpurkar is a Senior Research Analyst at OPEN Health. Her expertise includes conducting clinical, economic, and humanistic systematic literature reviews and targeted literature reviews to inform network meta-analyses, global value dossiers, and landscape assessments. She has worked on multiple therapeutic areas including oncology, diabetes, respiratory diseases, heart failure, neuroscience, and auto-immune diseases. She holds a Master’s degree in Pharmaceutical Manufacturing from Stevens Institute of Technology.
Stephan Martin is a Scientist at OPEN Health, supporting the Strategic Market Access team in literature reviews, payer research, strategy, evidence synthesis, project management, publication preparation, and medical communications in a variety of therapeutic areas. Stephan has therapeutic experience in the following areas: infectious disease, antimicrobial stewardship, oncology, epilepsy, rare diseases, and various others. He holds an MPH with a concentration in Epidemiology from Virginia Commonwealth University.
Omer Zaidi is a Senior Scientist at OPEN Health, His work focuses on systematic and targeted literature reviews, global value dossiers, AMCP dossiers, competitor and stakeholder analyses, value message communication, budget impact models, and cost-effectiveness analyses in a variety of therapeutic areas. Omer has therapeutic experience in oncology, infectious diseases, auto-immune diseases, diabetes, urology, respiratory diseases, and pain. He holds an MPH with a concentration in Health Policy from Yale University School of Public Health.
Cody Palmer is an accomplished mathematician specializing in ecological and infectious disease modeling and dynamical systems. He earned his degrees from the University of Nevada, Las Vegas, and the University of Montana, where he developed a robust understanding of complex mathematical applications in public health. Currently, Cody applies his expertise at Merck, where he focuses on supporting the value of HPV vaccination through data-driven insights and innovative modeling techniques. His work aims to enhance public awareness and policy regarding HPV prevention, ultimately contributing to global health initiatives.
Funding Statement
This publication(s) was sponsored by Merck & Co., Inc. All authors had full access to all the data and take complete responsibility for the integrity and accuracy of the data and analysis.
Disclosure statement
Marisa Felsher, Marcie Fisher-Borne, Tufail Malik, Wei Wang, and Cody Palmer are employees of Merck & Co., Inc. Nita Santpurkar, Stephan Martin, and Omer Zaidi are employees of OPEN Health, which received funding from Merck & Co., Inc. in connection with this publication(s).
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/21645515.2025.2516322.
Authorship
All named authors meet the International Committee of Medical Journal Editors criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Other contributors
Editorial assistance was provided by Christina DuVernay of OPEN Health, which received funding from Merck & Co., Inc., in connection with the publication(s).
Institutional review board statement
As this review is based on publication(s) already published, institutional review board approval is not applicable.
Data availability
The analysis reported herein relied only on publicly available data and information. All data used in this analysis are reported herein.
Ethical approval
As this review did not involve human participants, ethical approval did not apply to this publication(s).
References
- 1.Chesson HW, Dunne EF, Hariri S, Markowitz LE.. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex Transm Dis. 2014;41(11):660. doi: 10.1097/OLQ.0000000000000193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.de Sanjosé S, Diaz M, Castellsagué X, Clifford G, Bruni L, Muñoz N, Bosch FX. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis. Lancet Infect. Dis. 2007;7(7):453–35. doi: 10.1016/S1473-3099(07)70158-5. [DOI] [PubMed] [Google Scholar]
- 3.de Martel C, Plummer M, Vignat J, Franceschi S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int J Cancer. 2017;141(4):664–670. doi: 10.1002/ijc.30716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pešut E, Đukić A, Lulić L, Skelin J, Šimić I, Milutin Gašperov N, Tomaić V, Sabol I, Grce M. Human papillomaviruses-associated cancers: an update of current knowledge. Viruses. 2021;13(11):2234. doi: 10.3390/v13112234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.World Health Organization . Immunization, vaccines and biologicals: human papillomavirus vaccines (HPV). [accessed 2024 Nov 23]. https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases/human-papillomavirus-vaccines-(HPV).
- 6.World Health Organization . Human papillomavirus (HPV) vaccination coverage. [accessed 2024 Nov 22]. https://immunizationdata.who.int/global/wiise-detail-page/human-papillomavirus-(hpv)-vaccination-coverage?CODE=Global&ANTIGEN=&YEAR=.
- 7.Dykens JA, Peterson CE, Holt HK, Harper DM. Gender neutral HPV vaccination programs: reconsidering policies to expand cancer prevention globally. Front Public Health. 2023;11:1067299. doi: 10.3389/fpubh.2023.1067299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gavi-The Vaccine Alliance . Gender and immunisation. [accessed 2025 Apr 15]. https://www.gavi.org/our-alliance/strategy/gender-and-immunisation.
- 9.Xu MJ, Okerosi S, Nkya A, Van Loon K. Strategically striving to be more inclusive: a recommendation for gender-neutral human-papillomavirus vaccine policies. Hum Vaccin Immunother. 2025;21(1):2480404. doi: 10.1080/21645515.2025.2480404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cherif A, Ovcinnikova O, Palmer C, Engelbrecht K, Reuschenbach M, Daniels V. Cost-effectiveness of 9-valent HPV vaccination for patients treated for high-grade cervical intraepithelial neoplasia in the UK. JAMA Netw Open. 2024;7(10):e2437703. doi: 10.1001/jamanetworkopen.2024.37703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Arora S, Tuffaha H. Cost-effectiveness analysis of human papillomavirus vaccines for the prevention of cervical cancer in India. Asia Pac J Clin Oncol. 2024. Feb. 20(1):55–62. doi: 10.1111/ajco.13962. [DOI] [PubMed] [Google Scholar]
- 12.Ng SS, Hutubessy R, Chaiyakunapruk N. Systematic review of cost-effectiveness studies of human papillomavirus (HPV) vaccination: 9-valent vaccine, gender-neutral and multiple age cohort vaccination. Vaccine. 2018;36(19):2529–2544. doi: 10.1016/j.vaccine.2018.03.024. [DOI] [PubMed] [Google Scholar]
- 13.The World Bank. World Bank Country and Lending Groups . [accessed 2025 Apr 14]. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
- 14.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Canfell K, Kim JJ, Kulasingam S, Berkhof J, Barnabas R, Bogaards JA, Campos N, Jennett C, Sharma M, Simms KT, et al. HPV-FRAME: a consensus statement and quality framework for modelled evaluations of HPV-related cancer control. Papillomavirus Res. 2019;8:100184. doi: 10.1016/j.pvr.2019.100184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Husereau D, Drummond M, Augustovski F, de bekker-Grob E, Briggs AH, Carswell C, Caulley L, Chaiyakunapruk N, Greenberg D, Loder E, et al. Consolidated health economic evaluation reporting standards (CHEERS) 2022 explanation and elaboration: a report of the ISPOR CHEERS II good practices task force. Value Health. 2022;25(1):10–31. doi: 10.1016/j.jval.2021.10.008. [DOI] [PubMed] [Google Scholar]
- 17.Batista PM, Moreira TNF, Yen G, et al. Incremental public health and economic impact linked to higher vaccine coverage rate in a gender-neutral quadrivalent human papillomavirus vaccination program in Brazil. Value Health Reg Issues; Vol. 19. 2019; p. S43. doi: 10.1016/j.vhri.2019.08.245. [DOI] [Google Scholar]
- 18.de Mendonça Batista P, Chabrol Haas L, Moreira TNF, et al. PIN10 estimating the impact of a gender-neutral quadrivalent human papillomavirus vaccination program in all HPV6/11/16/18-related diseases in Brazil with a higher vaccine coverage rate. Value Health; Vol. 23. 2020; p. S170. doi: 10.1016/j.jval.2020.04.486. [DOI] [Google Scholar]
- 19.Carrasquilla M, Alvis-Zakzuk NJ, Zakzuk Sierra J, Gómez De la Rosa F, Beltran C, Rojas M, Prieto E, Yen G, Parellada C, Pavelyev A, et al. PIN13 estimating the impact of a gender-neutral quadrivalent human papillomavirus vaccination program in all HPV 6/11/16/18-related diseases in Colombia. Value Health. 2020;23:S170–S171. doi: 10.1016/j.jval.2020.04.489. [DOI] [Google Scholar]
- 20.Rendon AM, Barria L, Pavelyev A, Felsher M, Daniels V, Parellada C. EE329 public health and economic impact of a gender-neutral quadrivalent human papillomavirus vaccination program in El Salvador. Value Health. 2022;25(12):S119. doi: 10.1016/j.jval.2022.09.575. [DOI] [Google Scholar]
- 21.Pearson AL, Kvizhinadze G, Wilson N, Smith M, Canfell K, Blakely T. Is expanding HPV vaccination programs to include school-aged boys likely to be value-for-money: a cost-utility analysis in a country with an existing school-girl program. BMC Infect Dis. 2014;14(1):1–15. doi: 10.1186/1471-2334-14-351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sharma M, Sy S, Kim JJ. The value of male human papillomavirus vaccination in preventing cervical cancer and genital warts in a low-resource setting. BJOG. 2016;123(6):917–926. doi: 10.1111/1471-0528.13503. [DOI] [PubMed] [Google Scholar]
- 23.Tay SK, Hsu T-Y, Shcheprov A, Walia A, Kulkarni AS. The clinical and economic benefits of school-based quadrivalent HPV vaccination in Singapore. Int J Gynecology & Obstet. 2017;137(2):129–137. doi: 10.1002/ijgo.12126. [DOI] [PubMed] [Google Scholar]
- 24.Varga S, Lee Y, Sukarom I, Saxena K, Pavelyev A, Daniels VJ, Chen YT. POSB149 health impact and cost-effectiveness analysis of 9-valent versus bivalent HPV national immunization strategies in Singapore. Value Health. 2022;25(1):S89. doi: 10.1016/j.jval.2021.11.422. [DOI] [Google Scholar]
- 25.Wahab MT, Tan RKJ, Cook AR, Prem K. Impact of including boys in the national school-based human papillomavirus vaccination programme in Singapore: a modelling-based cost-effectiveness analysis. Vaccine. 2023;41(12):1934–1942. doi: 10.1016/j.vaccine.2023.02.025. [DOI] [PubMed] [Google Scholar]
- 26.Palmer C, Tobe K, Negishi Y, You X, Chen Y-T, Abe M. Health impact and cost effectiveness of implementing gender-neutral HPV vaccination in Japan. J Med Econ. 2023;26(1):1546–1554. doi: 10.1080/13696998.2023.2282912. [DOI] [PubMed] [Google Scholar]
- 27.Akyol Ersoy B, Koç E, Pavelyev A, Daniels V, Ugrekhelidze D, Malhan S, Basaran M, Ozyar E, Hafiz G, Yumuk PF, Selek U. EE286 cost effectiveness and public health impact of implementing gender-neutral vaccination with the 9-valent human papillomavirus vaccine in Turkiye. Value Health. 2023;26(12):S106. doi: 10.1016/j.jval.2023.09.552. [DOI] [Google Scholar]
- 28.Cheung TH, Cheng SSY, Hsu D, wing-Lei Wong Q, Pavelyev A, Sukarom I, Saxena K. Health impact and cost-effectiveness of implementing gender-neutral vaccination with the 9-valent HPV vaccine in Hong Kong. Hum Vaccines & Immunotherapeutics. 2023;19(2). doi: 10.1080/21645515.2023.2184605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Park J, Park J, Yang G, et al. Public health impact and the cost effectiveness of gender-neutral nonavalent human papillomavirus (9v-HPV) vaccination in South Korea. Infection and Chemotherapy; Vol. 55. 2023; p. S309–S310. doi: 10.3947/ic.2023.55.Suppl1. [DOI] [Google Scholar]
- 30.Olsen J, Jørgensen TR. Revisiting the cost-effectiveness of universal HPV-vaccination in Denmark accounting for all potentially vaccine preventable HPV-related diseases in males and females. Cost Eff Resour Alloc. 2015;13(1). doi: 10.1186/s12962-015-0029-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wolff E, Elfström KM, Cange HH, Larsson S, Englund H, Sparén P, Roth A. Cost-effectiveness of sex-neutral HPV-vaccination in Sweden, accounting for herd-immunity and sexual behaviour. Vaccine. 2018;36(34):5160–5165. doi: 10.1016/j.vaccine.2018.07.018. [DOI] [PubMed] [Google Scholar]
- 32.Diakite I, Nguyen S, Sabale U, Pavelyev A, Saxena K, Tajik AA, Wang W, Palmer C. Public health impact and cost-effectiveness of switching from bivalent to nonavalent vaccine for human papillomavirus in Norway: incorporating the full health impact of all HPV-related diseases. J Med Econ. 2023;26(1):1085–1098. doi: 10.1080/13696998.2023.2250194. [DOI] [PubMed] [Google Scholar]
- 33.Burger EA, Sy S, Nygård M, Kristiansen IS, Kim JJ, Liu X. Prevention of HPV-related cancers in Norway: cost-effectiveness of expanding the HPV vaccination program to include pre-adolescent boys. PLOS ONE. 2014;9(3):e89974. doi: 10.1371/journal.pone.0089974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Datta S, Pink J, Medley GF, Petrou S, Staniszewska S, Underwood M, Sonnenberg P, Keeling MJ. Assessing the cost-effectiveness of HPV vaccination strategies for adolescent girls and boys in the UK. BMC Infect Dis. 2019;19(1). doi: 10.1186/s12879-019-4108-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Owusu-Edusei K, Palmer C, Ovcinnikova O, Favato G, Daniels V. Assessing the health and economic outcomes of a 9-valent HPV vaccination program in the United Kingdom. JHEOR. 2022;9(1):140–150. doi: 10.36469/jheor.2022.34721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Daniels V, Saxena K, Patterson-Lomba O, Gomez-Lievano A, Saah A, Luxembourg A, Velicer C, Chen Y-T, Elbasha E. Modeling the health and economic implications of adopting a 1-dose 9-valent human papillomavirus vaccination regimen in a high-income country setting: an analysis in the United Kingdom. Vaccine. 2022;40(14):2173–2183. doi: 10.1016/j.vaccine.2022.02.067. [DOI] [PubMed] [Google Scholar]
- 37.Song Y, Choi W, Shim E. Cost-effectiveness of human papillomavirus vaccination in the UK: two versus single-dose of nonavalent HPV vaccination. Am J Prev Med. 2024. doi: 10.1016/j.amepre.2024.03.008. [DOI] [PubMed]
- 38.Teljeur C, Murchu EO, Harrington P, Ryan M. OP151 cost-utility of gender-neutral HPV vaccination in Ireland. Int J Technol Assess Health Care; Vol. 35. 2019; p. 34. doi: 10.1017/S0266462319001727. [DOI] [Google Scholar]
- 39.Boiron L, Joura E, Largeron N, Prager B, Uhart M. Estimating the cost-effectiveness profile of a universal vaccination programme with a nine-valent HPV vaccine in Austria. BMC Infect Dis. 2016;16(1). doi: 10.1186/s12879-016-1483-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bresse X, Goergen C, Prager B, Joura E. Universal vaccination with the quadrivalent HPV vaccine in Austria: impact on virus circulation, public health and cost–effectiveness analysis. Expert Rev Pharmacoecon Outcomes Res. 2014;14(2):269–281. doi: 10.1586/14737167.2014.881253. [DOI] [PubMed] [Google Scholar]
- 41.Palmer C, Dolk C, Sabale U, Wang W, Saxena K. Cost-effectiveness of nonavalent HPV vaccination in the Netherlands. Exp Rev Vaccines. 2024;23(1):312–323. doi: 10.1080/14760584.2024.2322543. [DOI] [PubMed] [Google Scholar]
- 42.Largeron N, Petry KU, Jacob J, Bianic F, Anger D, Uhart M. An estimate of the public health impact and cost-effectiveness of universal vaccination with a 9-valent HPV vaccine in Germany. Expert Rev Pharmacoecon Outcomes Res. 2017;17(1):85–98. doi: 10.1080/14737167.2016.1208087. [DOI] [PubMed] [Google Scholar]
- 43.Simoens S, Bento-Abreu A, Merckx B, Joubert S, Vermeersch S, Pavelyev A, Varga S, Morais E. Health impact and cost-effectiveness of implementing gender-neutral vaccination with the 9-valent human papillomavirus vaccine in Belgium. Front Pharmacol. 2021;12. doi: 10.3389/fphar.2021.628434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Majed L, Bresse X, El Mouaddin N, Schmidt A, Daniels VJ, Pavelyev A, Levy-Bachelot L, Elbasha E. Public health impact and cost-effectiveness of a nine-valent gender-neutral HPV vaccination program in France. Vaccine. 2021;39(2):438–446. doi: 10.1016/j.vaccine.2020.10.089. [DOI] [PubMed] [Google Scholar]
- 45.Haeussler K, Marcellusi A, Mennini FS, Favato G, Picardo M, Garganese G, Bononi M, Costa S, Scambia G, Zweifel P, Capone A, et al. Cost-effectiveness analysis of universal human papillomavirus vaccination using a dynamic bayesian methodology: the BEST II study. Value Health. 2015;18(8):956–968. doi: 10.1016/j.jval.2015.08.010. [DOI] [PubMed] [Google Scholar]
- 46.Mennini FS, Bonanni P, Bianic F, de Waure C, Baio G, Plazzotta G, Uhart M, Rinaldi A, Largeron N. Cost-effectiveness analysis of the nine-valent HPV vaccine in Italy. Cost Eff Resour Alloc. 2017;15(1). doi: 10.1186/s12962-017-0073-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Barbieri M, Boccalini S. Return on investment (ROI) of three vaccination programmes in Italy: HPV at 12 years, herpes zoster in adults, and influenza in the elderly. Nato Adv Sci Inst Se. 2023; 11(5):924. doi: 10.3390/vaccines11050924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Cherif A, Palmer C, Lombardi M, Boccalini S, Bechini A, Salvati C, Senese F. EE590 assessing health outcomes and cost-effectiveness of adult HPV vaccination in Italy. Value Health. 2023; 26(12):S166. doi: 10.1016/j.jval.2023.09.855. [DOI] [Google Scholar]
- 49.Laprise J-F, Drolet M, Boily M-C, Jit M, Sauvageau C, Franco EL, Lemieux-Mellouki P, Malagón T, Brisson M. Comparing the cost-effectiveness of two- and three-dose schedules of human papillomavirus vaccination: a transmission-dynamic modelling study. Vaccine. 2014;32(44):5845–5853. doi: 10.1016/j.vaccine.2014.07.099. [DOI] [PubMed] [Google Scholar]
- 50.Laprise J-F, Markowitz LE, Chesson HW, Drolet M, Brisson M. Comparison of 2-dose and 3-dose 9-valent human papillomavirus vaccine schedules in the United States: a cost-effectiveness analysis. J Infect Dis. 2016;214(5):685–688. doi: 10.1093/infdis/jiw227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Chesson HW, Ekwueme DU, Saraiya M, Dunne EF, Markowitz LE. The cost-effectiveness of male HPV vaccination in the United States. Vaccine. 2011;29(46):8443–8450. doi: 10.1016/j.vaccine.2011.07.096. [DOI] [PubMed] [Google Scholar]
- 52.Kim JJ, Goldie SJ. Cost effectiveness analysis of including boys in a human papillomavirus vaccination programme in the United States. BMJ. 2009;339():b3884. doi: 10.1136/bmj.b3884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Ortiz AP, Ortiz-Ortiz KJ, Ríos M, Laborde J, Kulkarni A, Pillsbury M, Lauschke A, Monsanto HA, Marques-Goyco C. Modelling the effects of quadrivalent human papillomavirus (HPV) vaccination in Puerto rico. PLOS One. 2017;12(11):e0184540. doi: 10.1371/journal.pone.0184540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Elbasha EH, Dasbach EJ, Insinga RP. A multi-type HPV transmission model. Bull Math Biol. 2008;70(8):2126–2176. doi: 10.1007/s11538-008-9338-x. [DOI] [PubMed] [Google Scholar]
- 55.Brisson M, Laprise J-F, Chesson HW, Drolet M, Malagón T, Boily M-C, Markowitz LE. Health and economic impact of switching from a 4-valent to a 9-valent HPV vaccination program in the United States. Research Support, Non-U.S. Gov’t Non-P.H.S. JNCIJ. 2016;108(1):djv282. doi: 10.1093/jnci/djv282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Choi SE, Choudhary A, Huang J, Sonis S, Giuliano AR, Villa A. Increasing HPV vaccination coverage to prevent oropharyngeal cancer: a cost-effectiveness analysis. Tumour Virus Res. 2022;13:200234. doi: 10.1016/j.tvr.2021.200234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Laprise J-F, Chesson HW, Markowitz LE, Drolet M, Martin D, Bénard É, Brisson M. Effectiveness and cost-effectiveness of human papillomavirus vaccination through age 45 years in the United States. Ann Intern Med. 2020;172(1):22–29. doi: 10.7326/M19-1182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Elbasha EH, Dasbach EJ. Impact of vaccinating boys and men against HPV in the United States. Vaccine. 2010;28(42):6858–6867. doi: 10.1016/j.vaccine.2010.08.030. [DOI] [PubMed] [Google Scholar]
- 59.Chesson HW, Laprise J-F, Brisson M, Markowitz LE. Impact and cost-effectiveness of 3 doses of 9-valent human papillomavirus (HPV) vaccine among US females previously vaccinated with 4-valent HPV vaccine. J Infect Dis. 2016;213(11):1694–1700. doi: 10.1093/infdis/jiw046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Daniels V, Prabhu VS, Palmer C, Samant S, Kothari S, Roberts C, Elbasha E. Public health impact and cost-effectiveness of catch-up 9-valent HPV vaccination of individuals through age 45 years in the United States. Hum Vaccines & Immunotherapeutics. 2021;17(7):1943–1951. doi: 10.1080/21645515.2020.1852870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Chesson HW, Meites E, Ekwueme DU, Saraiya M, Markowitz LE. Cost-effectiveness of nonavalent HPV vaccination among males aged 22 through 26 years in the United States. Vaccine. 2018;36(29):4362–4368. doi: 10.1016/j.vaccine.2018.04.071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Chesson HW, Meites E, Ekwueme DU, Saraiya M, Markowitz LE. Cost-effectiveness of HPV vaccination for adults through age 45 years in the United States: estimates from a simplified transmission model. Vaccine. 2020;38(50):8032–8039. doi: 10.1016/j.vaccine.2020.10.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Chesson HW, Markowitz LE, Hariri S, Ekwueme DU, Saraiya M. The impact and cost-effectiveness of nonavalent HPV vaccination in the United States: estimates from a simplified transmission model. Hum Vaccin Immunother. 2016;12(6):1363–1372. doi: 10.1080/21645515.2016.1140288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Kim JJ, Simms KT, Killen J, Smith MA, Burger EA, Sy S, Regan C, Canfell K. Human papillomavirus vaccination for adults aged 30 to 45 years in the United States: a cost-effectiveness analysis. PLOS Med. 2021;18(3):e1003534. doi: 10.1371/JOURNAL.PMED.1003534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Durham DP, Ndeffo-Mbah ML, Skrip LA, Jones FK, Bauch CT, Galvani AP. National- and state-level impact and cost-effectiveness of nonavalent HPV vaccination in the United States. Proc Natl Acad Sci USA. 2016;113(18):5107–5112. doi: 10.1073/pnas.1515528113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.De La Fuente J, Hernandez Aguado JJ, San Martín M, Ramirez Boix P, Cedillo Gómez S, López N. Estimating the epidemiological impact and cost-effectiveness profile of a nonavalent HPV vaccine in Spain. Hum Vaccin Immunother. 2019;15(7–8):1949–1961. doi: 10.1080/21645515.2018.1560770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Linertová R, Guirado-Fuentes C, Mar-Medina J, Teljeur C. Cost-effectiveness and epidemiological impact of gender-neutral HPV vaccination in Spain. Hum Vaccin Immunother. 2022;18(6):2127983. doi: 10.1080/21645515.2022.2127983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Yfantopoulos N, Gountas I, Sabale U, Pavelyev A, Skroumpelos A, Karokis A. EE385 cost effectiveness of gender-neutral vaccination with Gardasil 9 against HPV in Greece. Value Health. 2022;25(12):S131. doi: 10.1016/j.jval.2022.09.631. [DOI] [Google Scholar]
- 69.Qendri V, Bogaards JA, Baussano I, Lazzarato F, Vänskä S, Berkhof J. The cost-effectiveness profile of sex-neutral HPV immunisation in European tender-based settings: a model-based assessment. Lancet Public Health. 2020;5(11):e592–e603. doi: 10.1016/S2468-2667(20)30209-7. [DOI] [PubMed] [Google Scholar]
- 70.Kim JJ, Burger EA, Sy S, Campos NG. Optimal cervical cancer screening in women vaccinated against human papillomavirus. J Natl Cancer Inst. 2017;109(2):djw216. doi: 10.1093/jnci/djw216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Damm O, Horn J, Mikolajczyk RT, Kretzschmar MEE, Kaufmann AM, Deleré Y, Ultsch B, Wichmann O, Krämer A, Greiner W. Cost-effectiveness of human papillomavirus vaccination in Germany. Cost Eff Resour Alloc. 2017;15(1). doi: 10.1186/s12962-017-0080-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Ali HA, Hartner A-M, Echeverria-Londono S, Roth J, Li X, Abbas K, Portnoy A, Vynnycky E, Woodruff K, Ferguson NM, Toor J, et al. Vaccine equity in low and middle income countries: a systematic review and meta-analysis. Int J Equity Health. 2022;21(1):82. doi: 10.1186/s12939-022-01678-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Chaturvedi AK, Anderson WF, Lortet-Tieulent J, Curado MP, Ferlay J, Franceschi S, Rosenberg PS, Bray F, Gillison ML. Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers. J Clin Oncol. 2013;31(36):4550. doi: 10.1200/JCO.2013.50.3870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Zheng L, Wu J, Zheng M. Barriers to and facilitators of human papillomavirus vaccination among people aged 9 to 26 years: a systematic review. Sex Transm Dis. 2021;48(12):e255–e262. doi: 10.1097/olq.0000000000001407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kjaer SK, Nygård M, Dillner J, Brooke Marshall J, Radley D, Li M, Munk C, Hansen BT, Sigurdardottir LG, Hortlund M, et al. A 12-year follow-up on the long-term effectiveness of the quadrivalent human papillomavirus vaccine in 4 Nordic countries. Clin Infect Dis: Off Publ Infect Dis Soc Am. 2018;66(3):339–345. doi: 10.1093/cid/cix797. [DOI] [PubMed] [Google Scholar]
- 76.Hidayati NR, Endarti D, Setiawan D. The economic evaluation of HPV vaccination as a prevention of non-cervical cancer using modelling approaches: a systematic review. BIO web of conferences. 2023. doi: 10.1051/bioconf/20237505018. [DOI]
- 77.Lewis RM, Laprise JF, Gargano JW, Unger ER, Querec TD, Chesson HW, Brisson M, Markowitz LE. Estimated prevalence and incidence of disease-associated human papillomavirus types among 15- to 59-year-olds in the United States. Sex Transm Dis. 2021;48(4):273–277. doi: 10.1097/olq.0000000000001356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Hadj Yahia Mb B, Jouin-Bortolotti A, Dervaux B. Extending the human papillomavirus vaccination programme to include males in high-income countries: a systematic review of the cost-effectiveness studies. Clin Drug Investigation. 2015;35(8):471–485. doi: 10.1007/s40261-015-0308-4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The analysis reported herein relied only on publicly available data and information. All data used in this analysis are reported herein.